
Interesting Case October 2019
Case contributed by:
Bailey Hutchison, M.D. and Joseph Misdraji, M.D.
Massachusetts General Hospital Department of Pathology, Boston, MA
Clinical History
A 52-year-old female with a history of ankylosing spondylitis on immunosuppression presented with a 15-pound weight loss, fatigue, and night sweats over 4 months. Three years prior, she had undergone open heart mitral valve annuloplasty for rheumatic mitral valve stenosis. Laboratory investigation revealed pancytopenia, alkaline phosphatase of 1,070 U/mL, AST of 115 U/L and ALT of 51 U/L. Anti-smooth muscle antibody was positive. Angiotensin converting enzyme was 151 U/L (ULN 67 U/L). An MRI demonstrated splenomegaly. A viral hepatitis panel and tuberculosis screen prior to the initiation of immunosuppressive therapy had been negative. Liver and bone marrow biopsies were performed.
Pathologic Findings
Figure 1: Low power view of the liver biopsy shows marked sinusoidal congestion and steatosis.
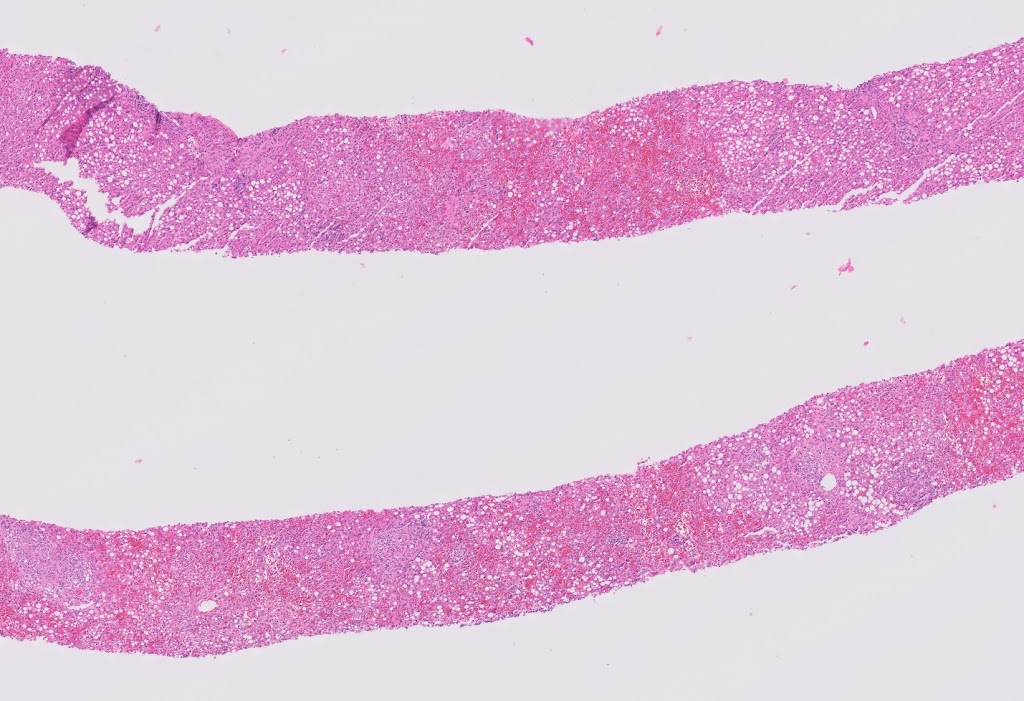 |
| Figure 1 |
Figure 2: Medium power view of the liver biopsy shows a granuloma (upper right) with a background of marked sinusoidal congestion with hepatic plate attenuation and steatosis.
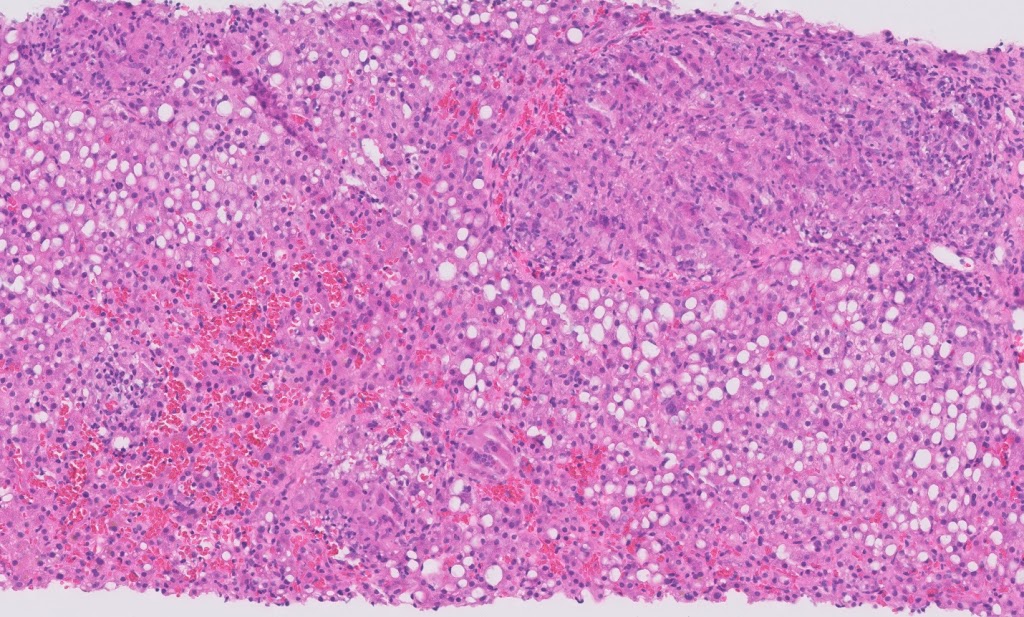 |
| Figure 2 |
Figure 3: High power view of the liver biopsy shows small non-necrotizing loose granuloma in a background of sinusoidal congestion and steatosis.
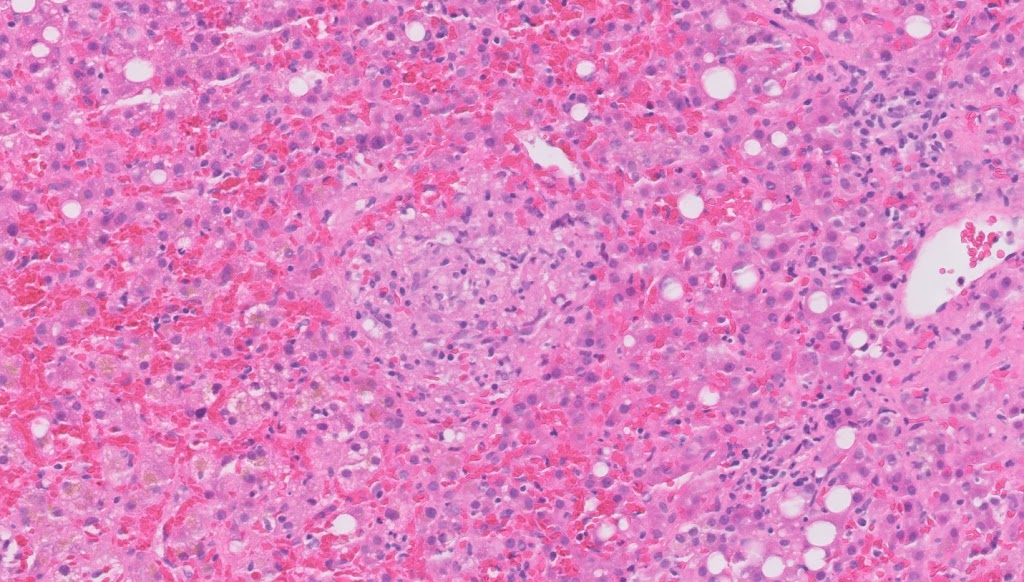 |
| Figure 3 |
Figure 4: High power view of the bone marrow biopsy shows a small granuloma.
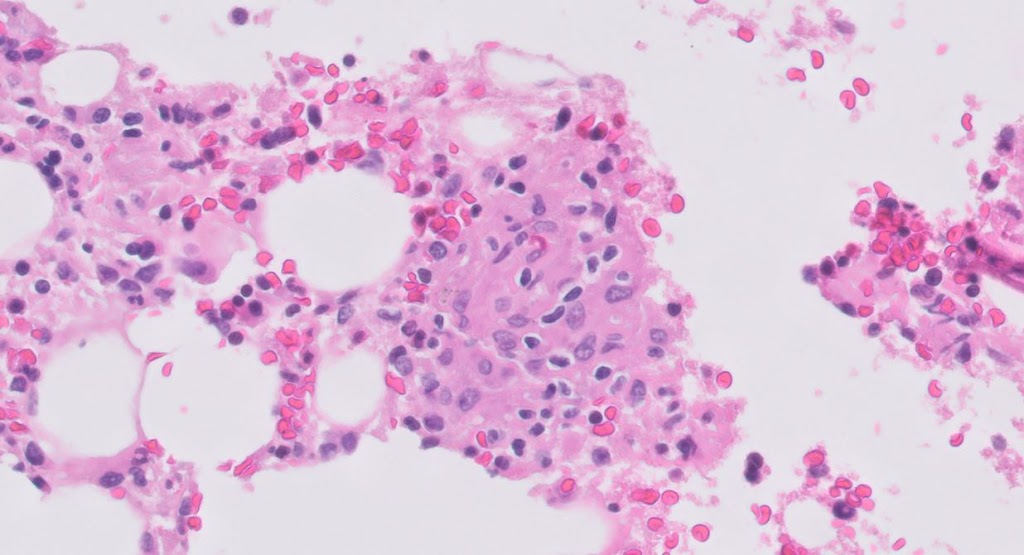 |
| Figure 4 |
Diagnosis
Disseminated non-tuberculous mycobacterial infection following cardiac surgery.
Discussion
Infection by non-tuberculous mycobacteria has been associated with contamination of medical instruments and potable water supplies in hospitals and other healthcare settings. Mycobacterium chimaera is the most widely known example, with numerous cases associated with contaminated heater-cooler water units used in cardiac surgery. Infection by or outbreaks of M. abscessus have also been reported, although the association with cardiac surgery is less clear than with M. chimaera.
M. chimaera is a species of the Mycobacterium avium complex which became notorious in 2015 when Sax and colleagues in Zurich reported 6 patients who had prosthetic valve endocarditis or vascular graft infections due to M. chimaera. An investigation pointed to contaminated heater-cooler water units used in open-heart surgery. It is believed that contamination occurred during the manufacturing process and during surgery, M. chimaera became aerosolized by the rear cooling fan and contaminated the surgical field. Since the original report, numerous cases have been reported. Because the latency period before symptomatic infection can be as long as 5 years (median 18 months), there is concern that the outbreak is not over. The most common clinical presentations of M. chimaera infection are cardiac manifestations (endocarditis, vascular graft infection, and mycotic aneurysm) or wound infections (mediastinitis and sternal wound infection), and most patients have prosthetic material that serves as a nidus for infection. Granulomatous disease that mimics sarcoidosis has been described, and patients are not infrequently inappropriately treated with immunosuppression for sarcoidosis or a presumed autoimmune disorder. In patients infected with M. chimaera, liver function tests typically show a biliary pattern of injury, with prominent alkaline phosphatase elevation and only mildly elevated aminotransferases.
The histologic features in the liver have been described in a small number of cases and include small ill-formed collections of histiocytes in sinusoids together with changes of venous outflow obstruction (e.g., sinusoidal dilation, congestion, and hepatic plate atrophy). Well-formed granulomas and giant cells are absent in reported cases. AFB stain is insensitive but PCR from tissue extracts can be positive. Culture remains the gold standard for diagnosis, and M. chimaera can be isolated from blood, urine, and affected body tissues.
In this case, despite the suspicion for M. chimaera, the organism was never able to be cultured. Instead, M. abscessus was cultured from an axillary lymph node. The patient was treated for disseminated mycobacterial infection for 18 months and her symptoms resolved. She underwent explant of the mitral valve annuloplasty ring with mitral valve replacement using homograft. A follow-up liver biopsy later showed mild cardiac-type fibrosis with resolution of granulomas.
References
1. Sax H, Bloemberg G, Hasse B, et al. Prolonged outbreak of Mycobacterium chimaera infection after open-chest heart surgery. Clin Infect Diseases. 2015;61:67-75
2. Kothavade RJ, Dhurat RS, Mishra SN, Kothavade UR. Clinical and laboratory aspects of the diagnosis and management of cutaneous and subcutaneous infections caused by rapidly growing mycobacteria. Eur J Clin Microbiol Infect Dis 2013;32:161-188.
3. Shafizadeh N, Hale G, Bhatnagar J, Alshak N, Nomura, J. Mycobacterium chimaerahepatitis: a new disease entity. Am J Surg Pathol 2019;43(2):244-250.
4. Schreiber PW, Hasse B, Sax H. Mycobacterium chimaera infections after cardiac surgery-lessons learned. Clin Microbiol Infect 2008;24 (11):1117-1118.
5. Scriven JE, Scobie A, Verlander NQ, Houston A, Collyns T, Cajic V, et al. Mycobacterium chimaera infection following cardiac surgery in the United Kingdom: clinical features and outcome of the first 30 cases. Clin Microbiol Infect 2018;24:1164-70.
6. Stammers AH, Riley JB. The heater cooler as a source of infection from nontuberculous mycobacteria. JECT 2016;48:55-59.
7. Baker AW, Lewis SS, Alexander BD, et al. Two-phase hospital-associated outbreak of Mycobacterium abscessus: Investigation and mitigation. CID 2017;64:902-911.