
Interesting Case April 2019
Case contributed by:
Madhavi Rayapudi, MD and Stephen C. Ward, MD, PhD
Department of Pathology, Icahn School of Medicine at Mount Sinai, New
York, NY
Clinical History:
55 year old female with past medical history of IgG lambda multiple myeloma diagnosed 3 years prior. She is status post multiple treatments and is currently in remission. She presents now with intermittent high fevers, dry cough, and elevated liver enzymes – AST 247 (Ref range 15-37IU/L); ALT 280 (Ref range 15-56 IU/L); Alkaline phosphatase 145 (Ref range 48-118 U/L); Bilirubin 0.5 (Ref range 0.2-1.5MG/DL). Liver biopsy was performed.
Microscopic Findings:
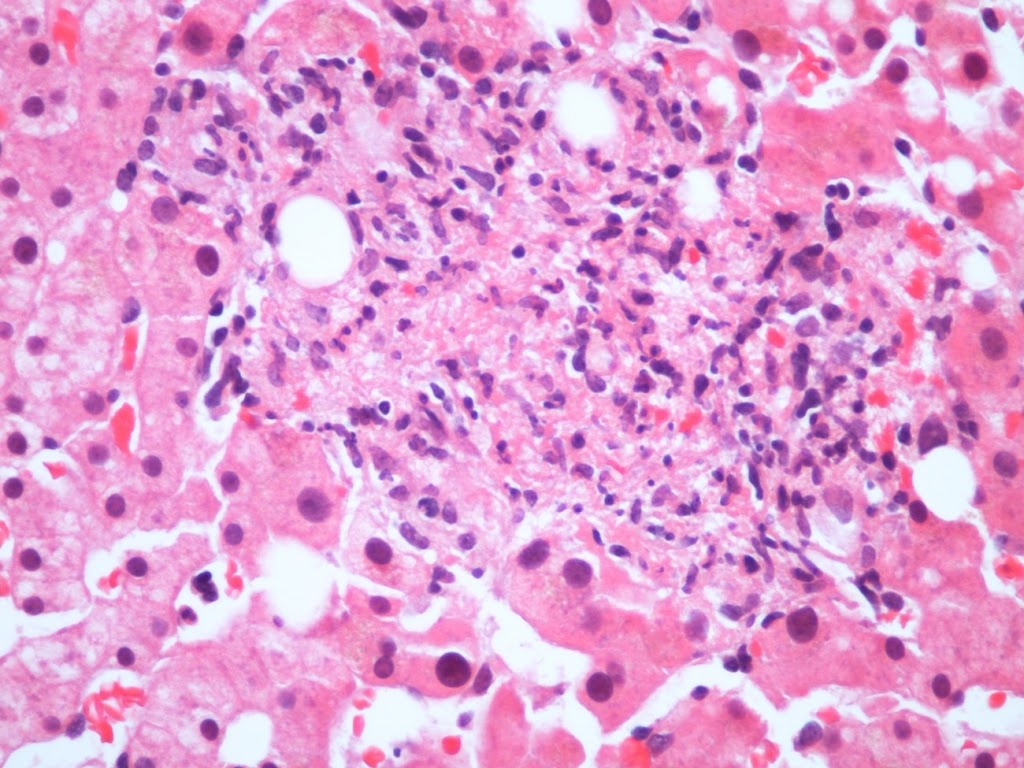
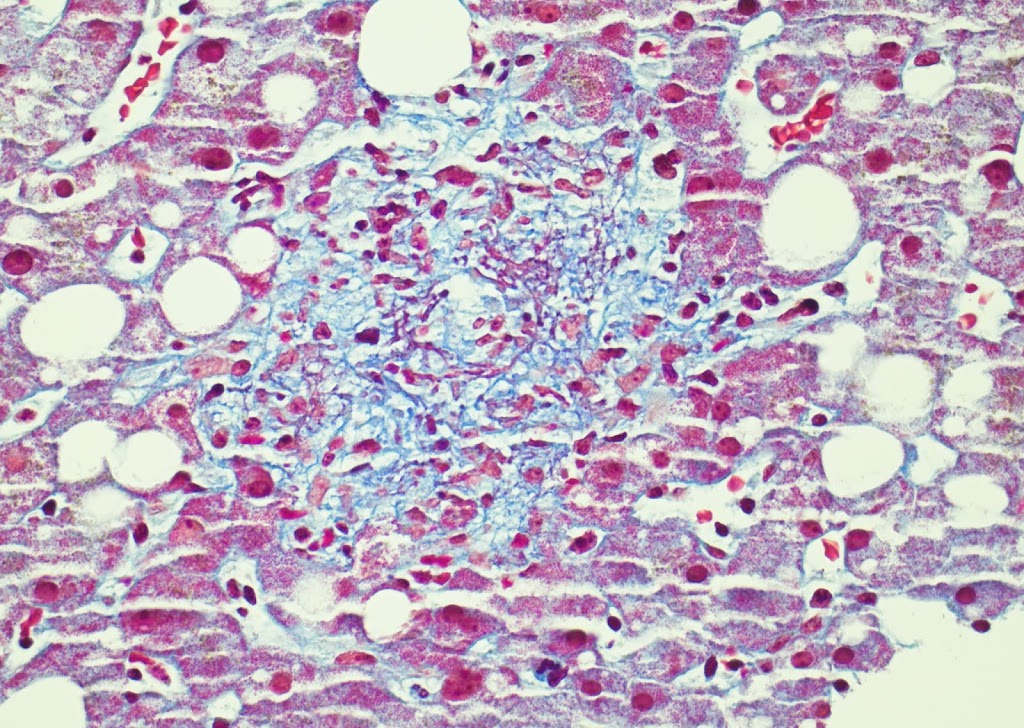
Liver needle biopsy specimen shows multiple nonnecrotizing granulomas predominantly located within the hepatic parenchyma. Several granulomas contain a lipid droplet, some with a loose ring of fibrin around the fat droplets (best seen on Masson trichrome stain). Mild macrovesicular steatosis without significant ballooning degeneration is also seen.
 |
| Figure 1 |
 |
| Figure 2 |
 |
| Figure 3 |
 |
| Figure 4 |
 |
| Figure 5 |
Diagnosis:
Granulomatous hepatitis with fibrin ring features secondary to immune checkpoint inhibitor toxicity.
The patient had been treated with venetoclax, ixazomib, dexamethasone, nelfinavir, and thalidomide. Immune checkpoint inhibitor therapy with anti-CTLA-4 agent ipilimumab and anti-PD-1 agent nivolumab was initiated three weeks prior to the biopsy. Following the biopsy the immune checkpoint inhibitor therapy was discontinued and liver enzymes returned to normal.
Discussion:
Immune checkpoint inhibitors have become standard of care in many types of malignancies; however, the underlying mechanism of hepatotoxicity is still not completely understood. In a retrospective study of 187 patients, an overall incidence of all grade hepatotoxicity with CTLA-4 inhibitors (e.g. ipilimumab) was 24%, 37% with PD-1 inhibitors (e.g. nivolumab), and 73% with the combination therapy (1). Immune check point inhibitor mediated hepatitis (ICIIMH) and idiopathic autoimmune hepatitis (iAIH) share some histologic similarities (2,3) but significant differences have also been described. ICIIMH was characterized by lobular hepatitis with abundant infiltration by CD3+ or CD8+ T-lymphocytes, while CD20+ or CD4+ lymphocytes were less likely to be seen in ICIIMH as compared to iAIH (4). Recently a granulomatous hepatitis with fibrin ring features has been described in patients treated with CTLA-4 inhibitors alone or in combination with PD-1 inhibitors. (5, 6). The granulomas consist of collections of epithelioid cells with a central lipid vacuole and a surrounding ring of fibrin. These cases also showed steatotosis with either spotty necrosis or perivenular confluent necrosis as well as central vein endotheliitis. Fibrin ring granulomas are not specific for immune checkpoint inhibitor toxicity. The differential diagnosis for fibrin ring granulomas also includes infection [Q fever (Coxiella burnetii), hepatitis A, visceral leishmaniasis, Epstein-Barr virus, toxoplasmosis, boutonneuse fever (Rickettsia conorii), staphylococcal infection, and salmonella], autoimmune (e.g. systemic lupus erythematosus), other drugs (e.g. allopurinol), Hodgkin disease, giant cell arteritis, metastases, as well as in the metabolic syndrome with hepatic steatosis, and mitochondrial injury (7, 8, 9).
References:
1. Shah N, Puthiamadathil J, Serzan M, et al. Clinical Outcome of immune related hepatitis (IrHep) in patients with advanced melanoma (AM) treated with single agent or combination immune checkpoint inhibitors (ICI) [abstract]. Ann Oncol. 2018 Oct; 29(8):viii433.
2. Kleiner DE, Berman D. Pathologic changes in ipilimumab- related hepatitis in patients with metastatic melanoma. Dig Dis Sci. 2012; 57:2233–2240.
3. Johncilla M, Misdraji J, Pratt DS, et al. Ipilimumab-associated Hepatitis. Am J Surg Pathol. 2015 Aug 1;39(8):1075–1084
4. Zen Y, Yeh MM. Hepatotoxicity of immune checkpoint inhibitors: a histology study of seven cases in comparison with autoimmune hepatitis and idiosyncratic drug-induced liver injury. Mod Pathol 2018; 31:965–973.
5. De Martin E, Michot JM, Papouin B, et al. Characterization of liver injury induced by cancer immunotherapy using immune checkpoint inhibitors. J Hepatol. 2018 Jun 1; 68(6):1181–1190.
6. Everett J, Srivastava A, Misdraji J. Fibrin ring granulomas in checkpoint inhibitor-induced hepatitis. Am J Surg Pathol. 2017; 41: 134–137.
7. Lewis JH. Chapter 40. Granulomas of the liver. In: Schiff ER, Maddrey WC, Reddy KR, editors Schiff’s disease of the liver. 12th ed. Wiley-Blackwell New Jersey, USA. 2018. p. 1028–1052.
8. Aguilar-Olivos N, Del Carmen Manzano-Robleda M, Gutiérrez-Grobe Y, et al. Granulomatous hepatitis caused by Q fever: a differential diagnosis of fever of unknown origin. Ann Hepatol. 2013 Jan 15; 12 (1):138–141.
9. Joseph J. Jennings, Rohan Mandaliya, Ahmad Nakshabandi & James H. Lewis (2019) Hepatotoxicity induced by immune checkpoint inhibitors: a comprehensive review including current and alternative management strategies, Expert Opinion on Drug Metabolism & Toxicology, 2019 15:3, 231-244, DOI: 10.1080/17425255.2019.1574744