
Interesting Case: January 2019
Case contributed by:
Phoenix D. Bell, MD, MS and Michael G. Drage, MD, PhD
University of Rochester Medical Center, Rochester, NY
Clinical History
A 3-year-old female with a past medical history of autism spectrum disorder and global developmental delay presented with several month history of decreased appetite, fatigue, and abdominal distension. A palpable abdominal mass was noted on physical exam. There was no history of nausea, abdominal pain, constipation, vomiting, or diarrhea. Serum alpha feto-protein (AFP), carcinoembryonic antigen (CEA), and beta-HCG were within normal limits.
Imaging Findings
An abdominal x-ray was performed, which showed striking hepatomegaly. Ultrasound demonstrated a multicystic mass (17.7 x 16.3 x 12.6 cm) in the right upper quadrant with thick septations and internal debris. MRI revealed mass effect on the adjacent structures, including upward displacement of the right hemidiaphragm and compression of the right kidney (Figures 1 and 2).
 |
| Figure 1 |
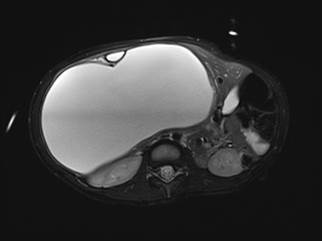 |
| Figure 2 |
Gross and Microscopic Findings
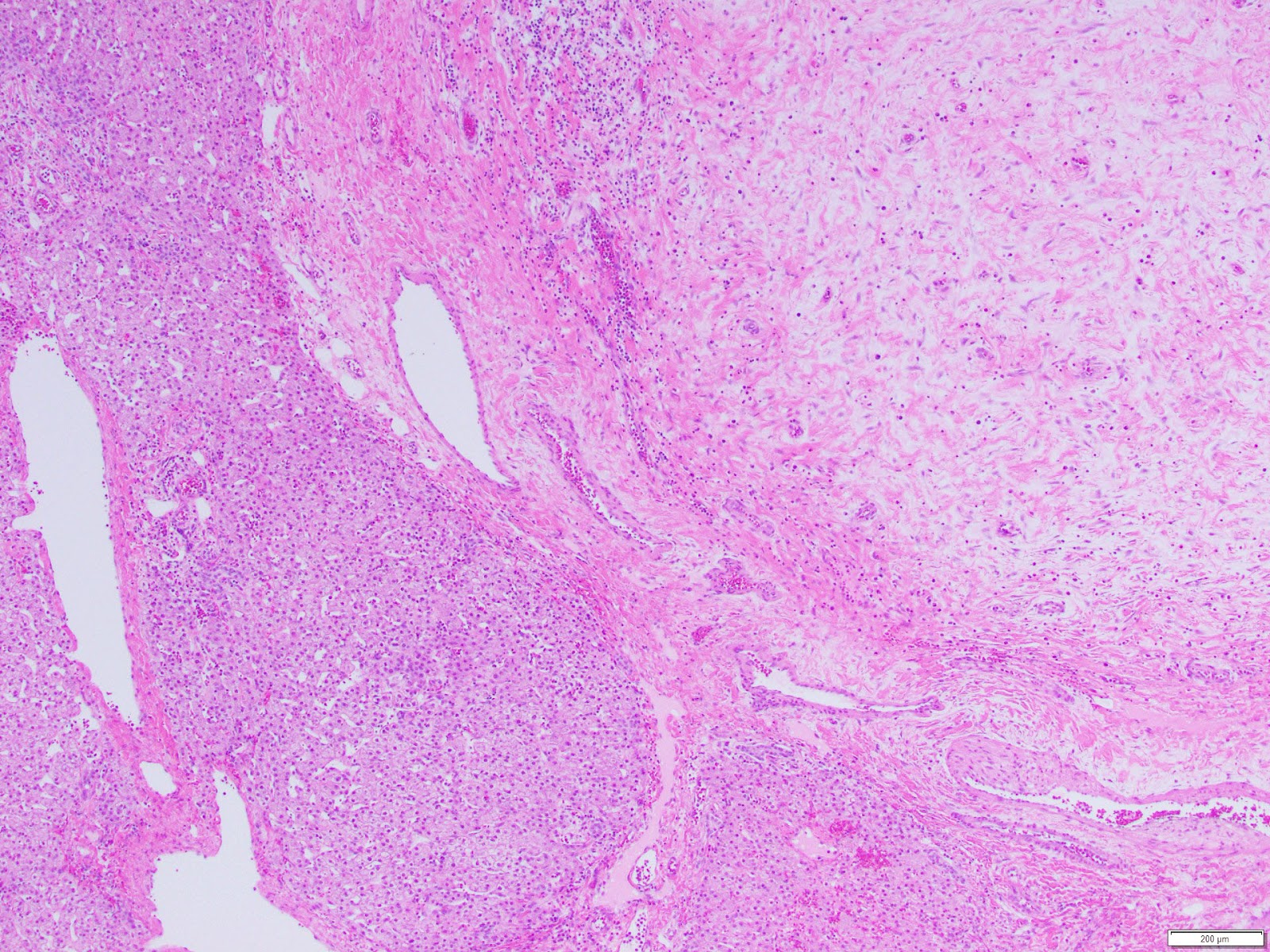
The patient underwent partial liver resection and gross examination showed an 18 x 17 x 5 cm, pink-purple cystic lesion. The cut surfaces were gray-white to pink-yellow with numerous cystic spaces up to 13.5 cm in greatest dimension and cross-sections revealing smaller intramural cysts (Figures 3 and 4). A portion of the specimen was sent for cytogenetic analysis, which failed due to lack of metaphase spreads. Microscopic examination revealed that the lesion was composed of a bland spindle cell population (Figure 5) within a variably loose, edematous, myxoid to hyalinized stroma with scattered ectatic thin-walled vessels, and occasional entrapped large biliary structures, the latter surrounded by dense concentric fibrosis (Figure 6). Grossly appreciated cystic structures were not lined by epithelium, and contained degenerated blood or bile (Figure 7), the latter often with xanthomatous reaction at the periphery (Figure 8). Cords of benign hepatocytes were prominent at the periphery of the lesion (Figure 9).
 |
| Figure 3 |
 |
| Figure 4 |
 |
| Figure 5 |
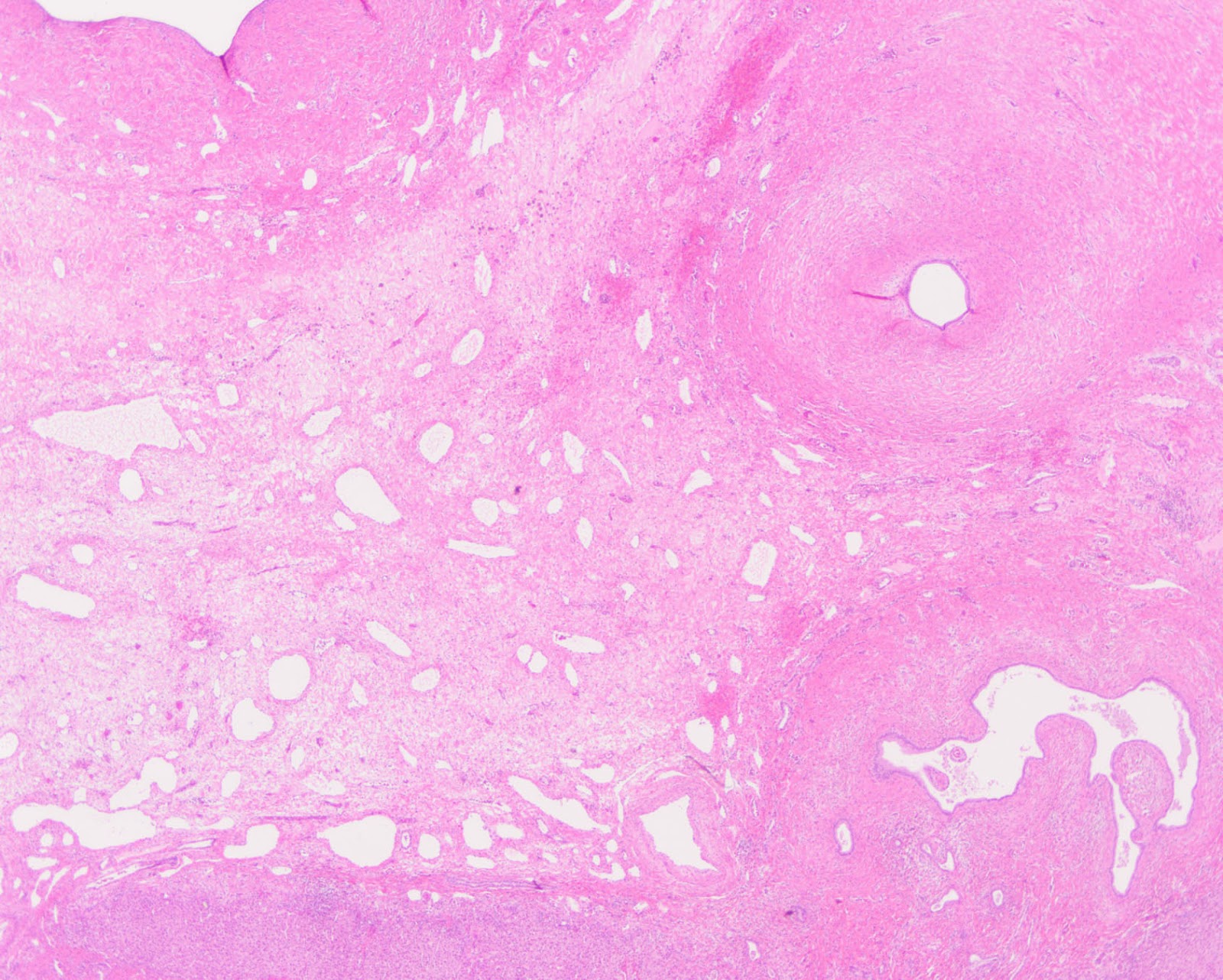 |
| Figure 6 |
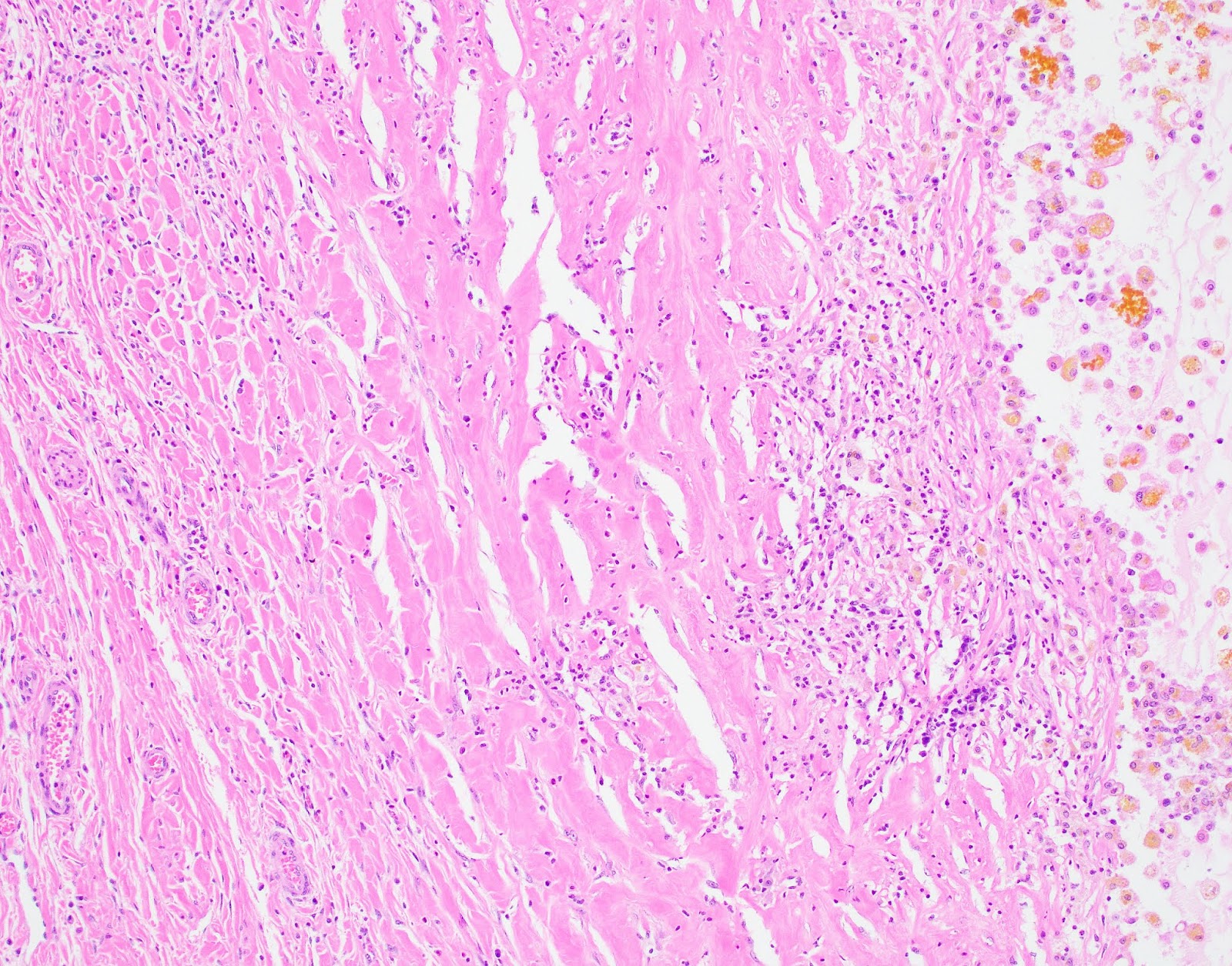 |
| Figure 7 |
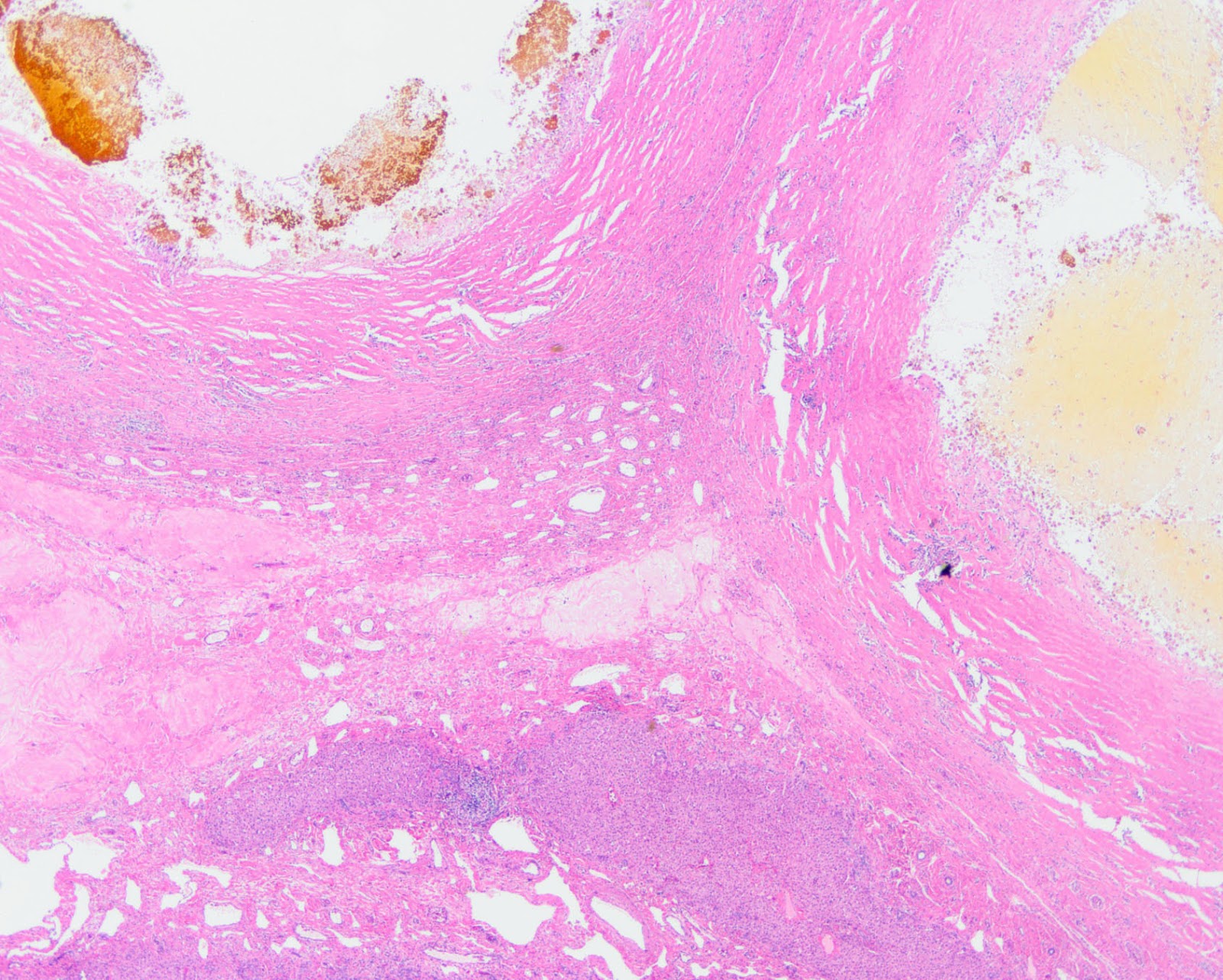 |
| Figure 8 |
 |
| Figure 9 |
Diagnosis
Hepatic mesenchymal hamartoma
Discussion
Hepatic mesenchymal hamartoma (HMH) represents 8% of primary liver tumors in children, and is the second most common benign pediatric liver tumor after infantile hemangioma [1-4]. Approximately 80% of MH present within the first two years of life as an asymptomatic, enlarging abdominal mass [5-7]. Approximately 75% occur in the right lobe [8]. Radiologic studies show variable solid and cystic components [5, 7]. Liver function tests are usually unremarkable[9]; however, there may be mild elevations in AFP[10]. Grossly, sectioning reveals soft cut surfaces with single to multiple cysts, which may contain clear-yellow to bilious fluid or gelatinous material [5, 6]. HMH has variable histologic features, which including areas of normal hepatic parenchyma separated by areas of spindled cells in a myxoid, collagenous, or hyalinized background[11]. The stroma contains interspersed elongated and clustered biliary ducts and numerous cystic spaces lacking an epithelial lining [3, 5]. A subset of HMH are discovered in adults, whose tumors show a greater tendency to be solid, densely fibrotic, and paucicellular [12], suggesting either involution of a long-standing lesion, or a different biology.
Occasionally, HMH may present as a solid lesion in children, altering the differential. Mixed epithelial-mesenchymal hepatoblastoma (HB), demonstrates radiologic and histologic overlap, particularly in areas of bland hepatocytes in a background of spindled cells. Elevated AFP and the presence of calcifications distinguish the latter from HMH [1, 2, 6].
Because of the age distribution and predilection for the right lobe, HMH was initially considered a developmental abnormality. Recent evidence has confirmed its neoplastic etiology. First, there are reports of synchronous or metachronous occurrence of HMH with undifferentiated embryonal sarcoma (UES), both of which share recurrent chromosomal rearrangements involving 19q13, with a translocation partner located at 11q11-3. In one case of concurrent HMH/UES, the lesions were contiguous and shared identical rearrangement in the stromal component [3], likely reflecting a somatic process. Dysregulated imprinting has also been proposed as a potential mechanism of tumorigenesis, based on observations that a subset of cases show evidence of androgenetic/biparental mosaicism [13], and interestingly, occasional cases are reported in patients with Beckwith-Wiedemann syndrome [14]. Although benign, HMH causes significant mass effect [14]. Complete resection is curative [1, 7]; liver transplant may be considered for unresectable cases [9, 11].
Learning Points
- MH is a rare tumor most often found in the pediatric population, which presents as an enlarging abdominal mass.
- Mixed epithelial-mesenchymal hepatoblastoma may demonstrate radiologic and histologic overlap with MH.
- Recent studies demonstrate that MH is a neoplastic process, rather than a developmental abnormality
Note: This case was presented in part at the College of American Pathologists Annual Meeting (Poster #94; Oct 21, 2018).
—————————-
References
1. Bahador, A., et al., Mesenchymal Hamartoma Mimicking Hepatoblastoma. International Journal of Organ Transplantation Medicine, 2014. 5(2): p. 78-80.
2. Kim, S.H., et al., Radiological Spectrum of Hepatic Mesenchymal Hamartoma in Children.Korean Journal of Radiology, 2007. 8(6): p. 498-505.
3. Mathews, J., E.J. Duncavage, and J.D. Pfeifer, Characterization of translocations in mesenchymal hamartoma and undifferentiated embryonal sarcoma of the liver. Experimental and Molecular Pathology, 2013. 95: p. 6.
4. Ishak, K.G., Z.D. Goodman, and J.T. Stocker, Tumors of the liver and intrahepatic bile ducts. 3rd Series. 2001, Washington D.C.: Armed Forces Institute of Pathology. 356.
5. Liao, W., et al., A 4 and a half years old boy with mesenchymal hamartomas in the left lateral lobe of the liver: A case report and literature review. Medicine, 2017. 96(31): p. e7281.
6. Patel, S.R., et al., Benign Hepatic Mesenchymal Hamartoma (HMH) – A Case Report. Journal of Clinical and Diagnostic Research : JCDR, 2014. 8(3): p. 119-120.
7. Rosado, E., et al., Mesenchymal hamartoma of the liver – a case report and literature review. Journal of Radiology Case Reports, 2013. 7(5): p. 35-43.
8. Stringer, M.D. and N.K. Alizai, Mesenchymal hamartoma of the liver: a systematic review. Journal of Pediatric Surgery, 2005. 40(11): p. 1681-1690.
9. Li, J., et al., Liver transplantation for a giant mesenchymal hamartoma of the liver in an adult: Case report and review of the literature. World journal of gastroenterology, 2015. 21(20): p. 6409-6416.
10. Iacob, E.R., et al., Mesenchymal hamartoma of the left liver lobe in an 18-month-old female patient. Rom J Morphol Embryol, 2016. 57(2 Suppl): p. 841-847.
11. Koganti, S.B., V.M. Thumma, and B. Nagari, Mesenchymal Hamartoma of the Liver: Complete Excision Always Necessary. Case Rep Surg, 2017. 2017: p. 8314102.
12. Cook, J.R., J.D. Pfeifer, and L.P. Dehner, Mesenchymal hamartoma of the liver in the adult: Association with distinct clinical features and histological changes. Human Pathology, 2002. 33(9): p. 893-898.
13. Lin, J., et al., Occult Androgenetic-Biparental Mosaicism and Sporadic Hepatic Mesenchymal Hamartoma. Pediatric and Developmental Pathology, 2011. 14(5): p. 360-369.
14. Pan, E.T., et al., Liver transplantation as definitive treatment of an unresectable mesenchymal hamartoma in a child with Beckwith-Wiedemann Syndrome. Journal of Surgical Case Reports, 2017. 8: p. 1-3.