
Interesting Case: April 2018
Case submitted by
Kalpesh Patel M.D. 1, Cassandra Gandle M.D. 2, Sadhna Dhingra M.D. 3
1. Department of Gastroenterology, Baylor College of Medicine, Houston TX
2. Department of Internal Medicine, Baylor College of Medicine, Houston TX
3. Department of Pathology and Immunology, Baylor College of Medicine, Houston TX
CLINICAL HISTORY
A 55 year-old Hispanic woman with rheumatoid arthritis, chronic back pain, disc prolapse and multiple surgeries on chronic opiate use, presents with chronic abdominal pain and rectal bleeding. Her gastric emptying studies were normal. Rectal bleeding was mild and secondary to hemorrhoids. Laboratory studies showed normal liver function tests, including normal transaminases and normal alkaline phosphatase. Urinalysis on multiple occasions over the past 3 years showed trace proteinuria. She underwent an esophagogastroduodenoscopy to rule out chronic pancreatitis.
ENDOSCOPIC FINDINGS
Endoscopic findings for esophagus, stomach and duodenum were normal. There were no endoscopic changes in common bile duct and pancreas. Endosonographic imaging showed diffuse abnormal echotexture in the left lobe of the liver. This was characterized by a hyperechoic appearance. EUS-FNA (fine needle biopsy) of the liver was performed.



LIVER BIOPSY FINDINGS
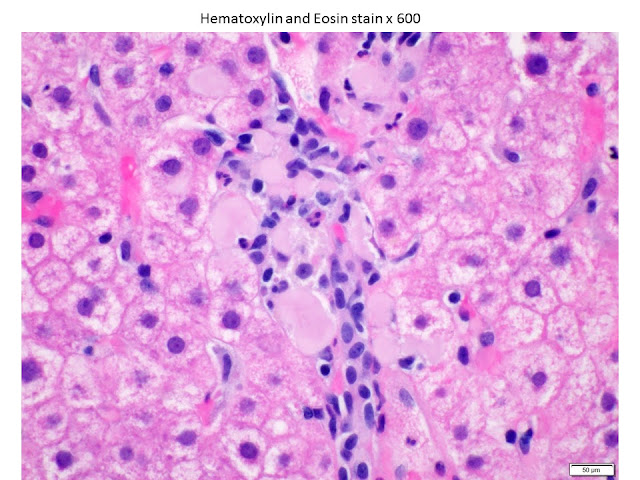
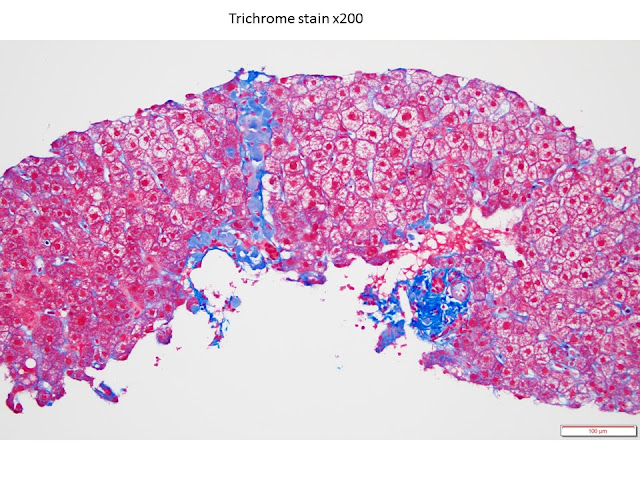
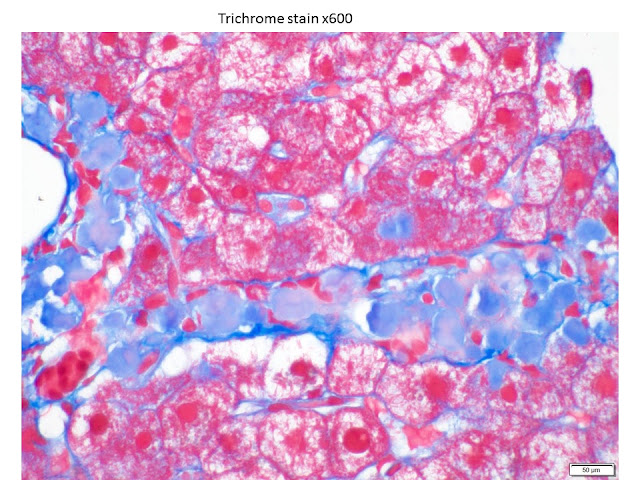
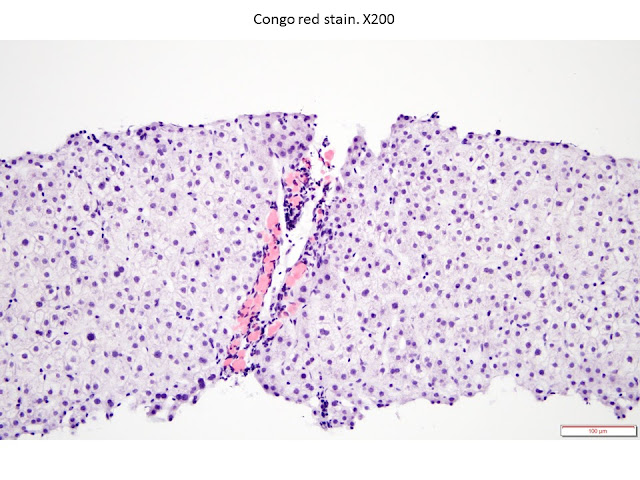
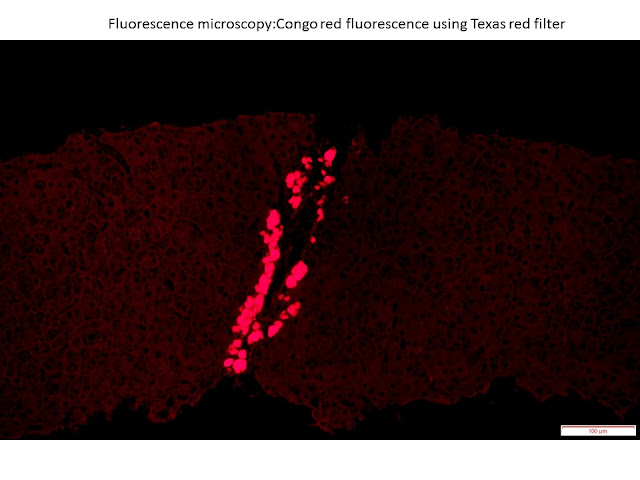
The liver biopsy showed multifocal amorphous globular eosinophilic deposits in a perivenular (zone 3) and portal/periportal distribution. These deposits were congophilic (congo red stain) and showed apple green birefringence on polarizing microscopy. The deposits also displayed fluorescence on fluorescent microscopy using Texas Red filter. The background liver parenchyma was unremarkable. No steatosis, lobular or portal inflammation was seen. No portal fibrosis was seen. The tissue was sent to Mayo Clinic Laboratories for mass spectroscopic analysis for accurate identification of amyloid. However, the amyloid deposition was minimal and insufficient for the mass spectroscopy to be performed. The diagnosis was based on the morphology and pattern of distribution.
DIAGNOSIS:
HEPATIC GLOBULAR AMYLOID, CONSISTENT WITH LEUCOCYTE-CELL DERIVED CHEMOTAXIN 2 – ASSOCIATED AMYLOIDOSIS (ALECT2)
HEPATIC GLOBULAR AMYLOID, CONSISTENT WITH LEUCOCYTE-CELL DERIVED CHEMOTAXIN 2 – ASSOCIATED AMYLOIDOSIS (ALECT2)
DISCUSSION
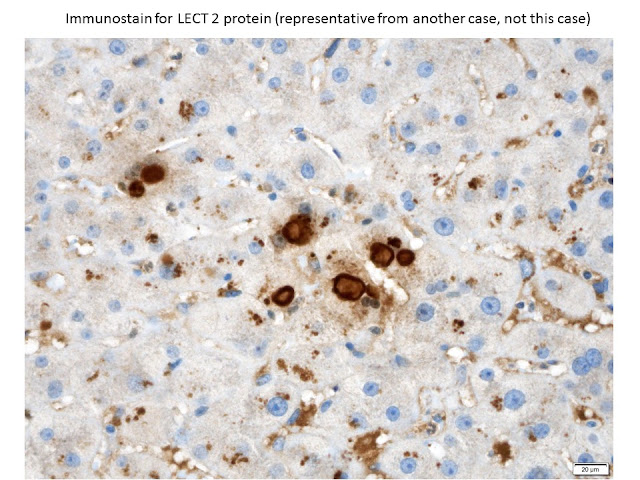
Liver is a frequent site of amyloid deposition in systemic amyloidosis. The most common type of amyloid deposition is AL (light chain-associated) amyloid or SAA (serum amyloid A) amyloid. We report a case of incidental hepatic ALECT2 in a hispanic female with clinical history significant for rheumatoid arthritis (RA). RA is a chronic inflammatory disease, which is usually associated with acute phase reactant serum amyloid A deposition in organs. Our patient had normal liver function tests and underwent an EUS-guided liver biopsy for abnormal echotexture while being evaluated for abdominal pain. The diagnosis of ALECT2 was made based on the morphology and pattern of distribution of amyloid deposition in the liver. Pure globular hepatic amyloid is specific for LECT2 amyloid. 1 Immunostain for LECT 2 using mouse monoclonal IgG antibody is highly specific and sensitive.
Leucocyte cell-derived chemotaxin 2 (LECT 2) is a relatively recently described amyloid protein first recognized in the international classification of amyloidosis in 2010. 2 It’s deposition was first described in the kidneys in 2008. 3 Although, abnormal amyloid bodies were noted in liver by Livni et al 4 as early as 1977, hepatic “globular’ amyloid deposition was first described in 1981. 5 The clinical significance of these deposits was unknown at the time of first description, and it was considered not to be distinctive from other systemic amyloidosis. 5, 6 In 2007, Makhlouf and Goodman, 7 reported globular hepatic amyloid in 9.6% of cases with hepatic amyloidosis, and hypothesized that this may represent an early form of liver involvement in generalized amyloidosis. Subsequently, the first case of hepatic ALECT2 was reported in 2014. 8 Chandan et al (2015) 1 reported that globular hepatic amyloid is highly sensitive and specific for ALECT2.
ALECT2 is associated with a distinctive clinical and pathological profile. It occurs in Hispanic patients with a median age range of 60.5 years and has female predilection. It has also been reported in other ethnic groups such as Punjabis (ethnic group in India and Pakistan), Arabs, Israelis, Native Americans and First Nation People from British Columbia. 9 The most common site of deposition is kidney and liver, but rare cases have been reported in spleen, small bowel, pancreas, gallbladder, parathyroid, prostate and lung. 10, 11 In contrast to AL amyloidosis or SAA amyloidosis, the presence of hepatic ALECT 2 is incidental, and not associated with abnormal liver function tests. 12 The pathogenesis of ALECT2 is unknown. The LECT2 protein is secreted by hepatocytes by the activation of LECT 2 gene present on chromosome 5q31.1. It is hypothesized that constitutive activation of gene or activation secondary to hepatocellular damage leads to secretion of LECT 2.
LEARNING POINT
ALECT2 (globular amyloid) is a recently described distinctive subtype of amyloid. This is seen in predominantly in Hispanic population with a male to female ratio of 0.6:1. It is an incidental finding in the liver biopsies. The amyloid deposition can be minimal/minute in some cases, and in this situation the demonstration of apple green birefringence of congophilic material by polarizing microscopy can be quite challenging. In this situation, congo red fluorescence using Texas Red filter increases the diagnostic yield. 13 Based on the current literature, at the time of reporting of this case, hepatic ALECT2 is not associated with clinically significant liver disease. However, in kidneys it is associated with slowly progressive chronic renal disease without systemic disease. Therefore, a nephrology consultation may be a consideration when this is first detected in liver biopsies. Knowledge and identification of this specific amyloid is important to avoid unnecessary administration of toxic therapeutic drugs for AL or AA amyloid.
References
1. Chandan VS, Shah SS, Lam-Himlin DM, Petris GD, Mereuta OM, Dogan A, Torbenson MS, Wu TT. Globular hepatic amyloid is highly sensitive and specific for LECT2 amyloidosis. Am J Surg Pathol. 2015 Apr;39(4):558-64.
2. Sipe JD, Benson MD, Buxbaum JN, Ikeda S, Merlini G, Saraiva MJ, Westermark P. Amyloid fibril protein nomenclature: 2010 recommendations from the nomenclature committee of the International Society of Amyloidosis. Amyloid. 2010 Sep;17(3-4):101-4.
3. Benson MD, James S, Scott K, Liepnieks JJ, Kluve-Beckerman B. Leukocyte chemotactic factor 2: A novel renal amyloid protein. Kidney Int. 2008 Jul;74(2):218-22.
4. Livni N, Behar AJ, Lafair JS. Unusual amyloid bodies in human liver. Ultrastructural and freeze-etching studies. Isr J Med Sci. 1977;13:1163–1170.
5. French SW, Schloss GT, Stillman AE. Unusual amyloid bodies in human liver. Am J Clin Pathol. 1981 Mar;75(3):400-2.
6. Kanel GC, Uchida T, Peters RL. Globular hepatic amyloid–an unusual morphologic presentation. Hepatology. 1981 Nov-Dec;1(6):647-52.
7. Makhlouf HR, Goodman ZD. Globular hepatic amyloid: an early stage in the pathway of amyloid formation: a study of 20 new cases. Am J Surg Pathol. 2007 Oct;31(10):1615-21
8. Damlaj M, Amre R, Wong P, How J. Hepatic ALECT-2 amyloidosis causing portal hypertension and recurrent variceal bleeding: a case report and review of the literature. Am J Clin Pathol. 2014 Feb;141(2):288-91
9. Nasr SH, Dogan A, Larsen CP. Leukocyte Cell-Derived Chemotaxin 2-Associated Amyloidosis: A Recently Recognized Disease with Distinct Clinicopathologic Characteristics. Clin J Am Soc Nephrol. 2015 Nov 6;10(11):2084-93.
10. Said SM, Sethi S, Valeri AM, Chang A, Nast CC, Krahl L, Molloy P, Barry M, Fidler ME, Cornell LD, Leung N, Vrana JA, Theis JD, Dogan A, Nasr SH. Characterization and outcomes of renal leukocyte chemotactic factor 2-associated amyloidosis. Kidney Int. 2014 Aug;86(2):370-7.
11. Khalighi MA, Yue A, Hwang MT, Wallace WD. Leukocyte chemotactic factor 2 (LECT2) amyloidosis presenting as pulmonary-renal syndrome: a case report and review of the literature. Clin Kidney J. 2013 Dec;6(6):618-21.
12. Mereuta OM, Theis JD, Vrana JA, Law ME, Grogg KL, Dasari S, Chandan VS, Wu TT, Jimenez-Zepeda VH, Fonseca R, Dispenzieri A, Kurtin PJ, Dogan A. Leukocyte cell-derived chemotaxin 2 (LECT2)-associated amyloidosis is a frequent cause of hepatic amyloidosis in the United States. Blood. 2014 Mar 6;123(10):1479-82.
13. Clement CG, Truong LD. An evaluation of Congo red fluorescence for the diagnosis of amyloidosis. Hum Pathol. 2014 Aug;45(8):1766-72