Clinical History
The patient is a 32-year old woman G3P2 who suffered a miscarriage after her first child.
Imaging Findings
MRI reveals an ill-defined, heterogeneously T2 hyperintense, right lobe liver segment 7/8 lesion, without washout. The mass measures 4.0 x 3.4cm and has been stable since 2014. The background liver is within normal limits.
Liver Biopsy Findings
February and June 2015 needle core biopsies were performed. Provided for review are two parts of core needle biopsies obtained from 2015. The first core needle biopsy from February of 2015, site unspecified consists of three portal tracts without significant fibrous expansion. No steatosis or significant histopathologic findings are seen. The second specimen labeled mid lesion #2 shows quite different histopathologic findings of striking sinusoidal dilation and corresponding hepatocyte atrophy (see Figure 1).
There is one vascular structure with fibrin within the lumen. No significant macrovesicular steatosis or inflammation is seen in either of the two liver biopsies. There are focal areas of hemorrhage and other areas with hepatocyte dropout. Another liver biopsy was obtained from the patient four months later in June of 2015. Again, striking zone 3 hepatocellular atrophy and sinusoidal dilatation was seen (Figure 2.) Fibrin was identified in several of the portal venules (Figure 3).
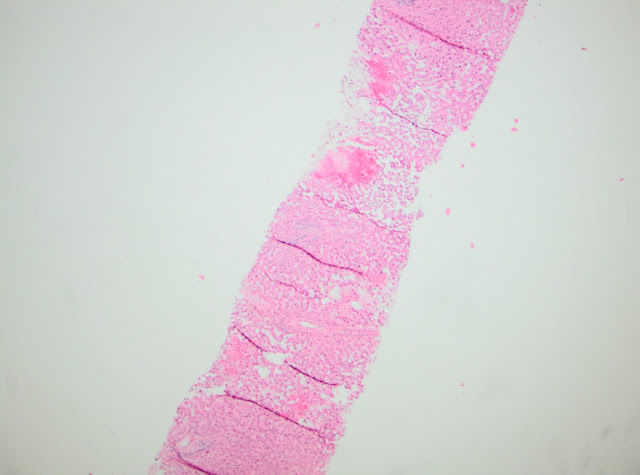 |
| Figure 1. February 2015 biopsy 20X. |
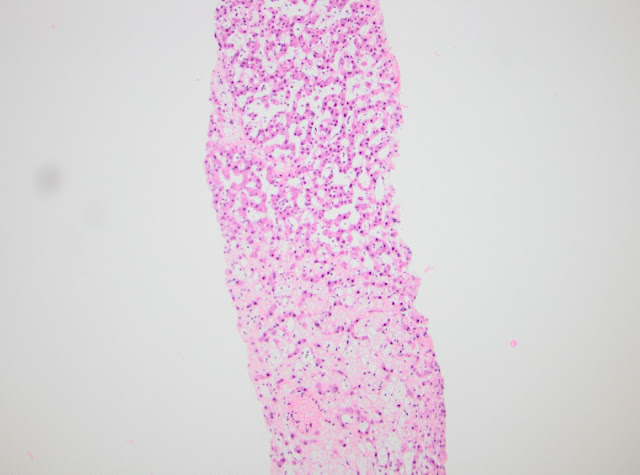 |
| Figure 2. June 2015 biopsy 100X |
 |
| Figure 3. June 2015 biopsy 200X |
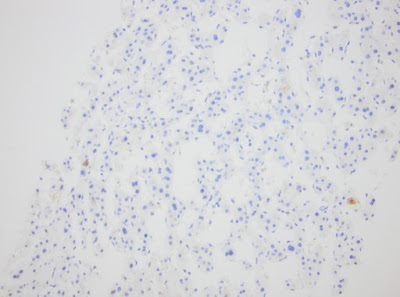
As a mass lesion has been demonstrated on radiologic evaluation, a panel of immunohistochemical stains were performed to further evaluate the possibility of a hepatic adenoma. CRP is interpreted as negative. No loss of LAFB was seen. Heat shock protein 70 (HSP70) is negative and no nuclear staining is seen using Beta-Catenin. CD34 highlights the vessels within the portal tracts and fails to stain in the area with the dilated sinusoids. Glutamine Synthetase shows the typical zone 3 pattern of staining.
Diagnosis and Discussion
• Striking zones 2 and 3 sinusoidal dilation with corresponding hepatocyte atrophy
• Focal hemorrhage and hepatocyte dropout.
• See comment
Prior to discussing this challenging case, please note that this patient’s liver biopsies were reviewed by several prominent hepatopathologists and their respective diagnoses were not necessarily in concert. Upon careful review, maintenance of the portal tracts are seen, but the spacing of the portal tracts is irregular. The histopathology varies between the two specimen parts from the biopsies from February of 2015, with one being relatively unremarkable hepatic parenchyma and the other demonstrating hepatocellular atrophy and sinusoidal dilatation. There are areas with hepatocyte dropout. The hepatic biopsy from June of 2015 shows similar histopathologic findings with sinusoidal dilation.
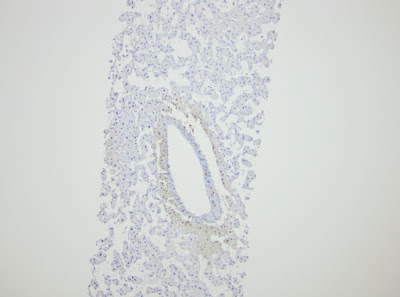
The panel of immunohistochemical stains were quite helpful in the evaluation for hepatic adenoma. CRP (Figure 4) is interpreted as negative and therefore, the diagnosis of telangiectatic adenoma is not supported. LAFBP retained staining and therefore, type 1 hepatic adenoma is not supported. In addition, the absence of macrovesicular steatosis does not support this diagnosis. Heat shock protein 70 (Figure 6) is negative and no nuclear staining is seen using Beta-Catenin. CD34 (Figure 7) highlights the vessels within the portal tracts and fails to stain in the area with the dilated sinusoids. Glutamine Synthetase (Figure 8) shows the typical zone 3 pattern of staining, and therefore, the diagnosis of focal nodular hyperplasia is not supported.
 |
| Figure 4. C-reactive protein (CRP) immunostain. |
 |
| Figure 5. LAFBP immunostain. |
 |
| Figure 6. HSP immunostain. |
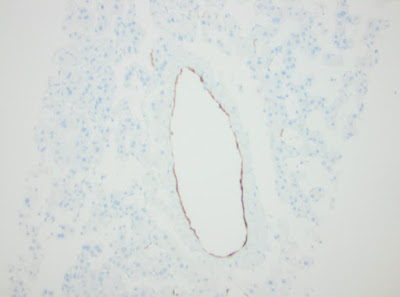 |
| Figure 7. CD34 immunostain. |
 |
| Figure 8. Glutamine synthetase immunostain. |
Given the histopathologic findings and immunophenotypic staining pattern, the diagnosis of adenoma or focal nodular hyperplasia is not supported. There is the possibility that these parenchymal changes are that of tissue adjacent to a mass lesion. Therefore, sampling cannot be completely excluded.
The differential diagnoses of histopathologic findings of striking sinusoidal dilation with corresponding hepatic atrophy can be seen in hypercoagulable states, mass lesion, vascular injury, infectious etiologies, or adverse drug reaction. A hypercoagulable workup was suggested for this patient. Other causes of hypercoagulability include oral contraceptive use and hematologic malignancies. Congestive heart failure and constrictive pericarditis can result in this histopathologic picture, but given the young age of this patient and per findings in the electronic medical record, the likelihood of these etiologies were less likely.
Major Learning Points
- A mass lesion in the liver does not always represent a neoplasm. The possibility of vascular flow abnormality need be entertained.
- Pause before making a diagnosis of hepatic adenoma in the presence of portal triads.
- Performance of a battery of immunohistochemical stains is immensely helpful in diagnosing or excluding hepatic adenoma and focal nodular hyperplasia.
References
Odze and Goldblum Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas, 3rd Edition, Robert Odze and John Goldblum, Philadelphia, PA, © 2015 by Saunders, an imprint of Elsevier IncSaunders.
MacSween’s Pathology of the Liver, SIXTH EDITION, Alastair D. Burt, Bernard C. Portmann and Linda D. Ferrell. New York, © 2012, Elsevier Limited.
This case was submitted by:
Erin Rubin, MD, FCAP, James Park Dewar, MD, Professorship of Pathology, Department of Pathology, University of Oklahoma School of Medicine, Oklahoma City, OK
