
Interesting Case October 2015
Clinical History:
An obese sixty year old gentleman with a history of GERD and hypertension presented to an emergency room with repeated bouts of sharp unremitting right upper quadrant pain over a one year period. Imaging findings during clinical workup (see below) revealed changes concerning for gallbladder adenocarcinoma. A biliary stent was placed, and the patient was referred to a tertiary center for further management. Exploratory laparotomy demonstrated an indurated gallbladder which was densely adherent to the porta hepatis and the interface between segments 4B and 5. A cholecystectomy and resection of the aforementioned liver segments was performed for presumed adenocarcinoma of the gallbladder.
Labs:
At initial evaluation: AST, 474; ALT, 358; alkaline phosphatase, 268; INR, 1.1
Imaging:
CT scan demonstrated heterogeneity of the fundus of the gallbladder and multiple benign hepatic cysts. MRI and MRCP showed and thickened gallbladder wall with dilation and beading of the biliary tree but no evidence of common bile duct stones. The clinical differential included malignancy, adenomyomatosis, inflammation, and infection.
Cholecystectomy and Liver Segmentectomy Findings:
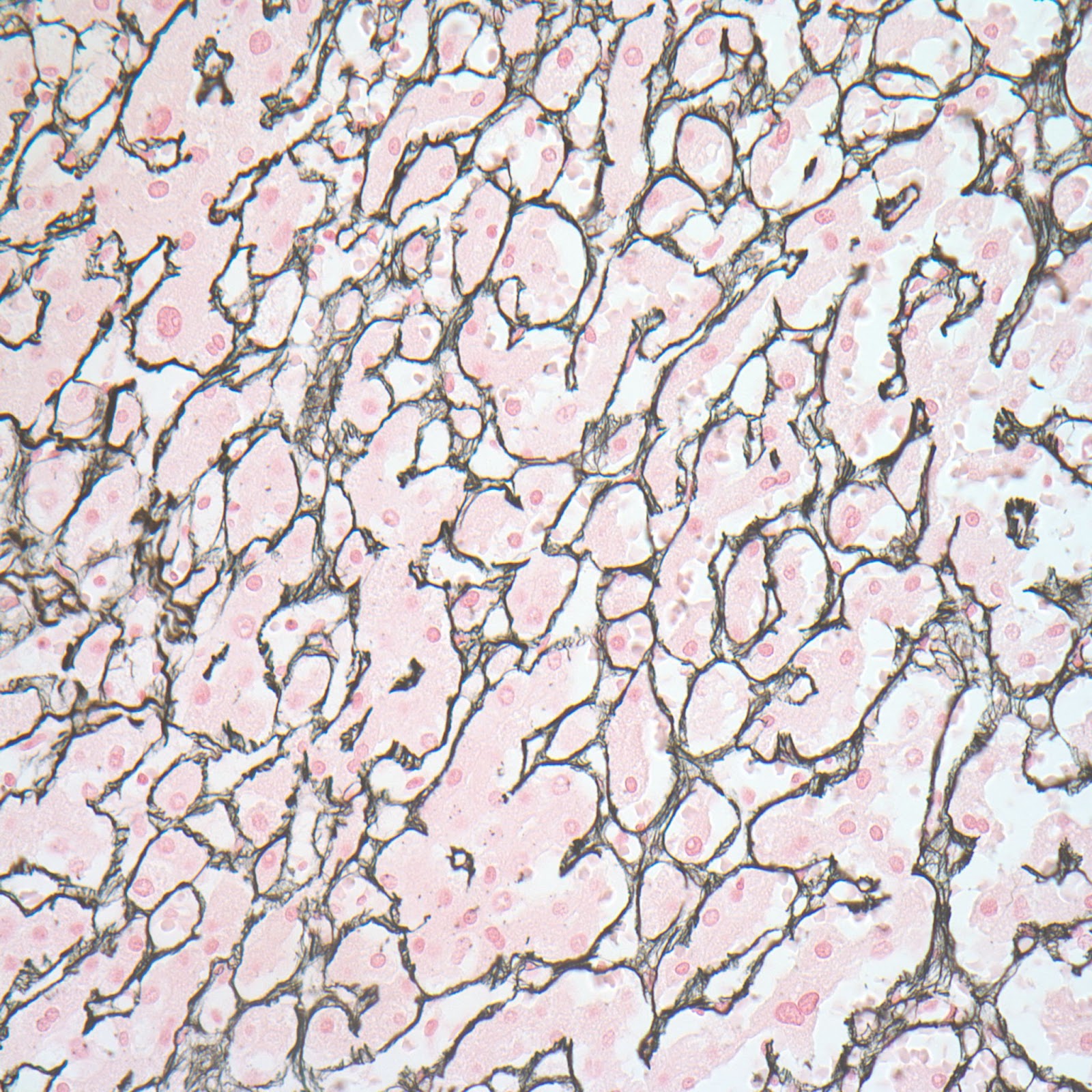
Sections of the gallbladder demonstrated a marked chronic inflammatory infiltrate with numerous germinal centers and plasma cells involving the lamina propria and muscularis mucosa, with focal involvement of the submucosa (Figures 1&2). The submucosa was fibrotic. Immunohistochemistry demonstrated polytypic plasma cells with clusters of up to 40 IgG4 positive plasma cells per 40x field (Figure 3). The superficial gallbladder wall demonstrated scattered IgG4 plasma cells and the deeper, more fibrotic portions of the gallbladder wall demonstrated prominent clusters of IgG4 positive plasma cells. The surface epithelium showed mild reactive changes but no dysplasia. Sections of the liver segmentectomy showed normal architecture. Portal areas contained mild to moderate chronic inflammatory infiltrates. A few portal areas demonstrated prominent clusters of lymphocytes. Many portal areas did not contain a portal vein branch and in one septal portal area there was fibrous obliteration of the vein (Figure 4, white arrow). The parenchyma demonstrated atrophy of zone 3 hepatocytes (blue arrow) compatible with portal vein compromise (Figure 5).
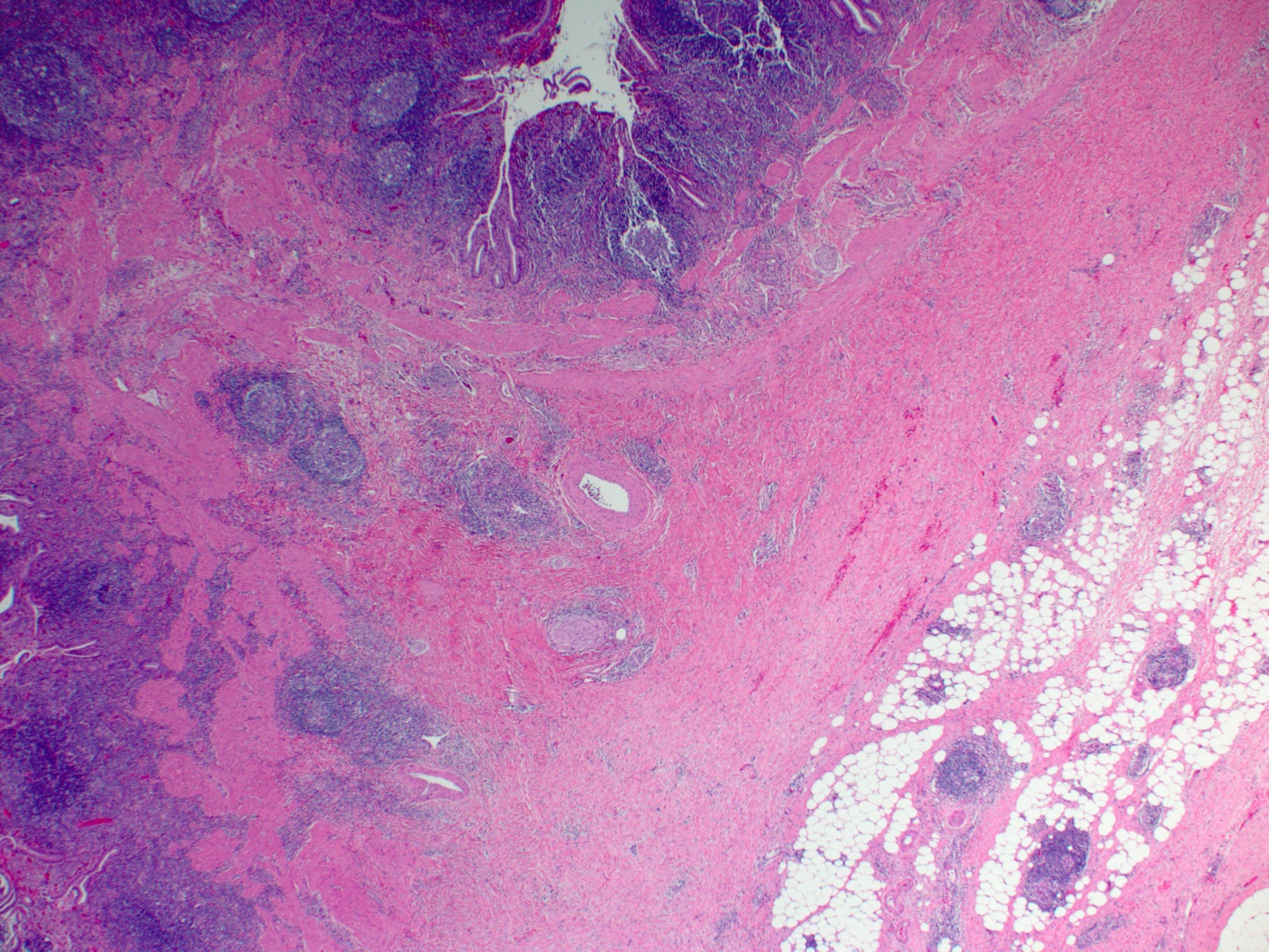 |
| Figure 1 |
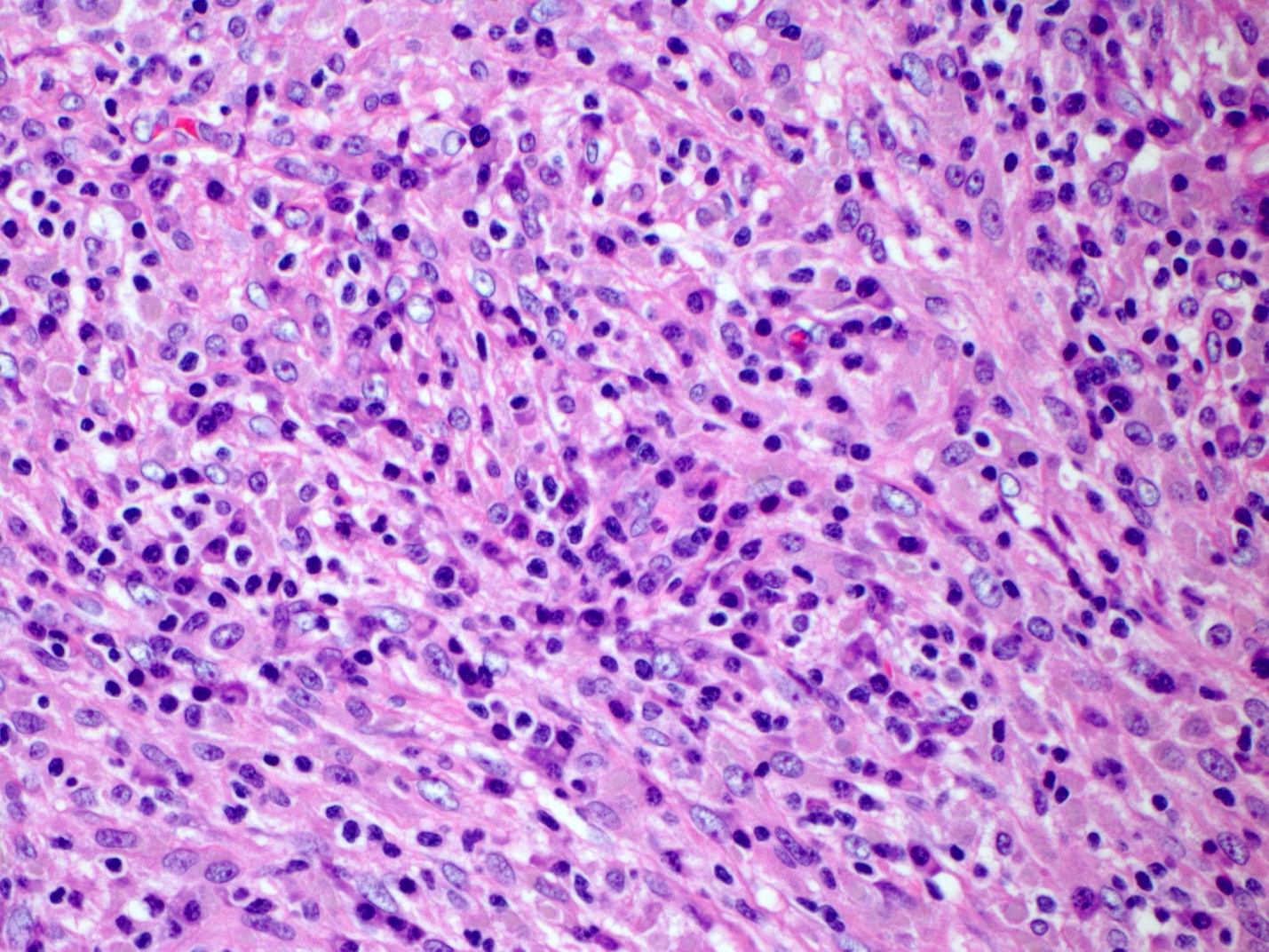 |
| Figure 2 |
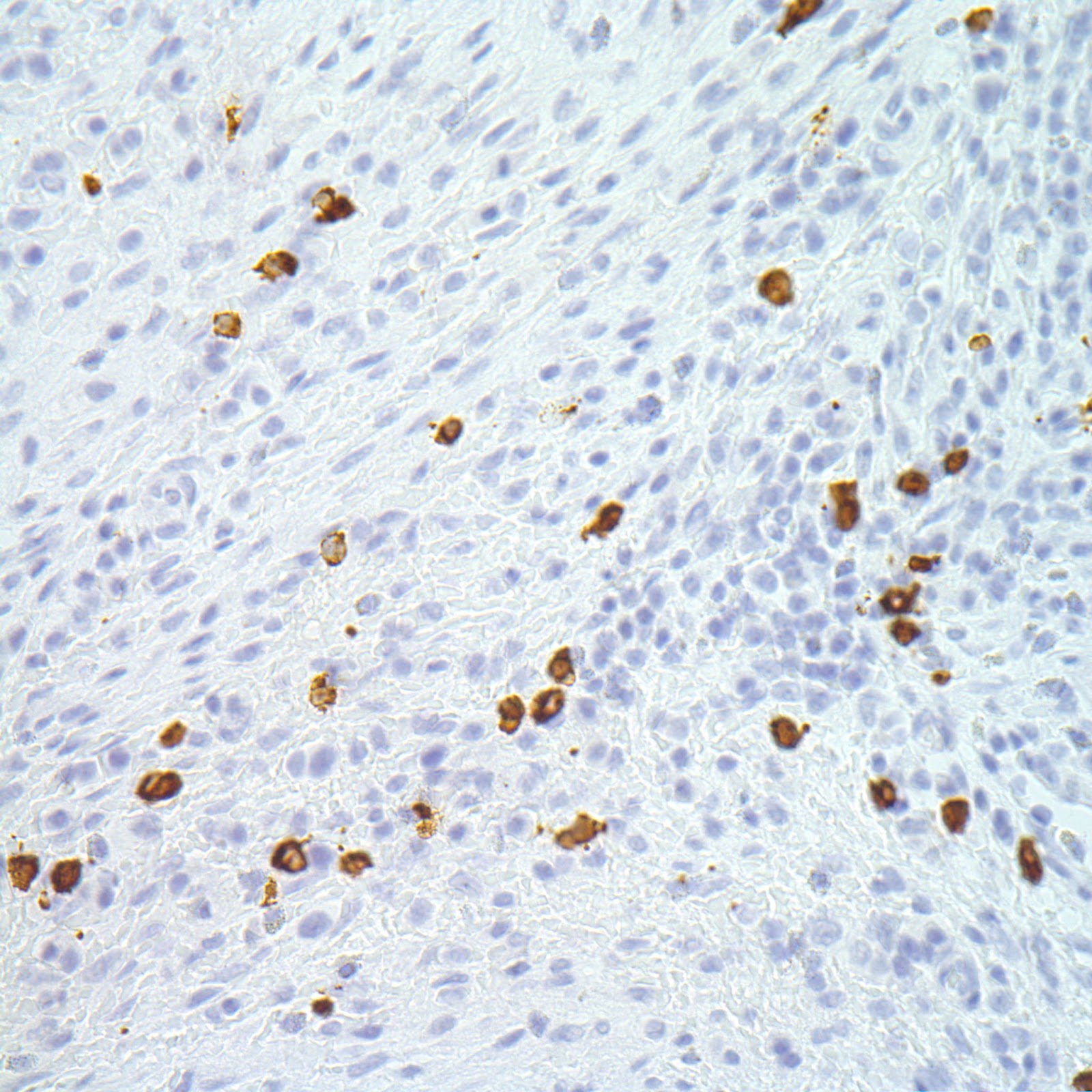 |
| Figure 3 |
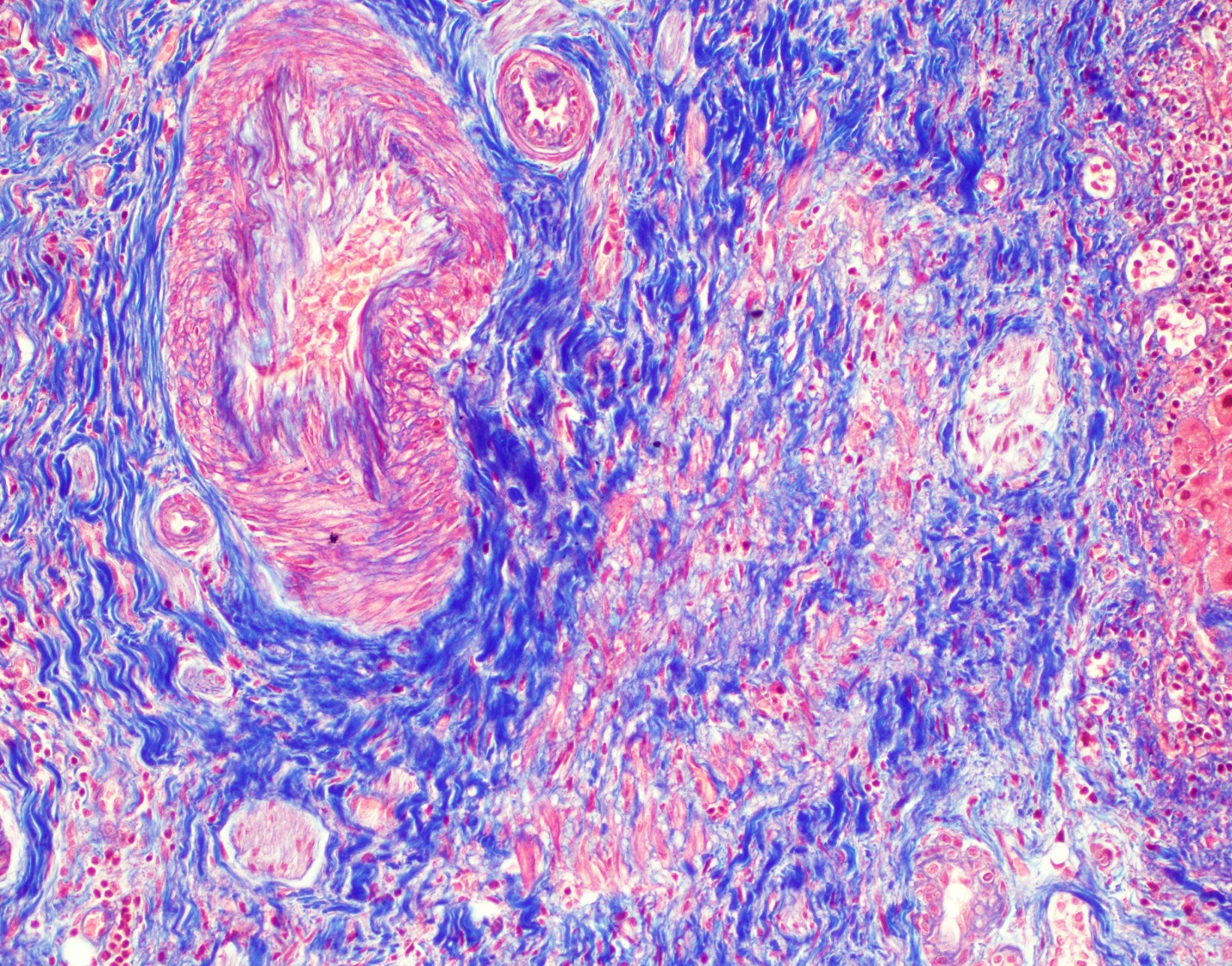 |
| Figure 4 |
 |
| Figure 5 |
Diagnosis:
Chronic cholecystitis consistent with IgG4 sclerosing disease with sclerosing portal venopathy.
No dysplasia or carcinoma.
Discussion:
Immunoglobulin G4 (IgG4)-related disease is a fibroinflammatory condition that is characterized by tumor-like swelling of involved organs, due to a dense lymphoplasmacytic infiltrate with numerous IgG4 positive plasma cells, a “storiform” pattern of fibrosis, eosinophilia, obliterative phlebitis, and in most cases elevated serum IgG4 concentrations above the upper limit of normal (>135 ng/dL) (N Engl J Med. 2012 Feb;366(6):539-51). IgG4-related disease has been described in essentially every organ system, including the biliary tree. It typically occurs in middle-aged men, especially in association with conditions such as type 1 (IgG4-related) autoimmune pancreatitis (AIP), IgG4-related tubulointerstitial nephritis, and retroperitoneal fibrosis. However, the proportion of female patients appear to be significantly higher than in men with respect to head and neck manifestations of the disease, such as IgG4-related sialadenitis and IgG4-related ophthalmic disease (Am J Surg Pathol. 2010;34(12):1812).
IgG4-related sclerosing cholangitis is the second most common manifestation of the disease, second only to type 1 autoimmune pancreatitis (AIP). The percentage of patients with AIP who have extrahepatic bile duct involvement is estimated to be between 71-100%, and rarely occurs in the absence of pancreatitis (Curr Opin Rheumatol. 2011;23(1):57). It is imperative to distinguish IgG4-related cholangitis from primary sclerosing cholangitis since the former is typically responsive to steroid therapy (Gastroenterology. 2008 Mar;134(3):706-15). Inflammatory bowel disease and cholangiocarcinoma, both of which are associated with primary sclerosing cholangitis, has not been reported in patients with IgG4-related sclerosing cholangitis (Curr Opin Gastroenterol. 2008;24(3):389). The presence of clinical manifestations in extra-biliary organs, histomorphological findings such as IgG4 positive plasma cells, storiform interstitial fibrosis, and responsiveness to steroids, can all help differentiate these two entities.
IgG4-related sclerosing cholangitis in the absence of AIP is rare, and as in the current case, can mimic extrahepatic cholangiocarcinoma. It is seen primarily in middle to older age men. A recent study compared material from patients with IgG4-related sclerosing cholangitis without AIP, to those with IgG4-related sclerosing cholangitis and AIP, and to those with extrahepatic cholangiocarcinoma, primary sclerosing cholangitis, and secondary sclerosing cholangitis. The histomorphologic features that helped distinguish IgG4-related sclerosing cholangitis from these other entities include a marked degree of bile duct injury, higher percentage of lymphoid follicle formation, a higher percentage of perineuritis, as well as a more diffuse and dense lymphoplasmacytic infiltrate. The authors also found that the presence of more than 50 IgG4-positive plasma cells per high power field in a biopsy specimen was sufficient to exclude cholangiocarcinoma. Therefore biopsy specimens with fewer than 50 IgG4 positive plasma cells did not adequately exclude the presence of unsampled cholangiocarcinoma (Scand. J. Gastroenterol. 2015 Apr;50(4):447-453)
Case Contributed by:
Ramir Arcega, MD and Charles Lassman, MD, Ph.D.
UCLA David Geffen School of Medicine