
Interesting Case June 2015 #2
Case History:
A 62 year old woman with a history of renal cell carcinoma removed years ago presented with a 2.4 cm liver mass found in CT during follow-up. A partial hepatectomy was performed.
Laboratory values:
ALT, AST, alkaline phosphatase and bilirubin were normal. There is no prior history of liver disease.
Gross examination of the liver resection:
Cut section reveals a 2.4 cm circumscribed mass with a gray-brown focally spongy appearance.
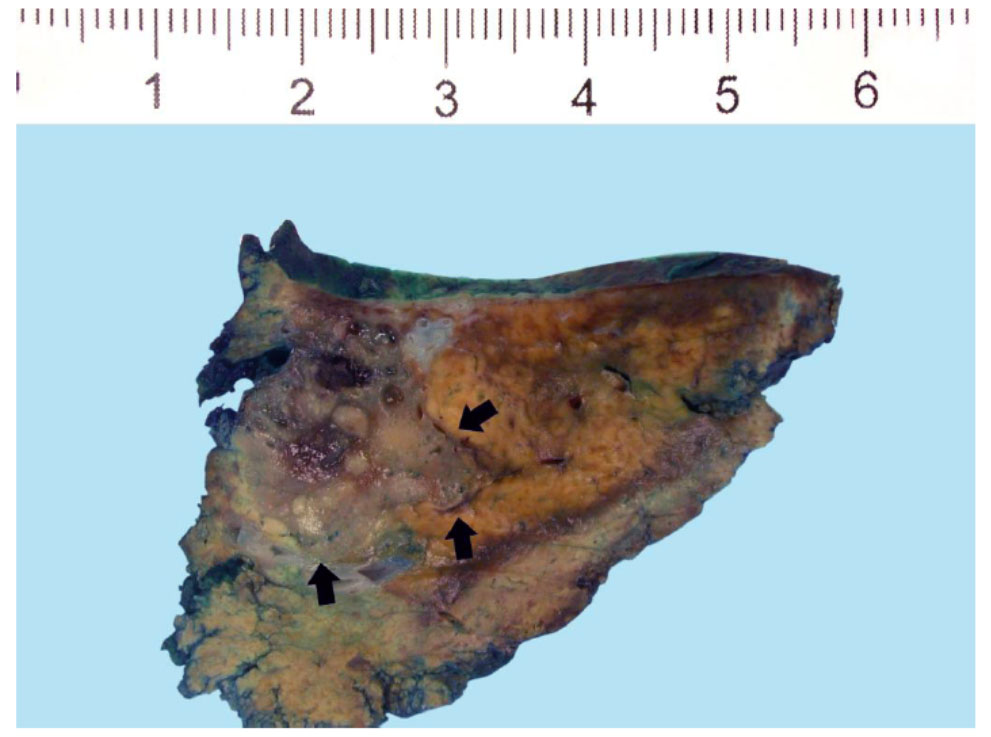 |
| Figure 1 |
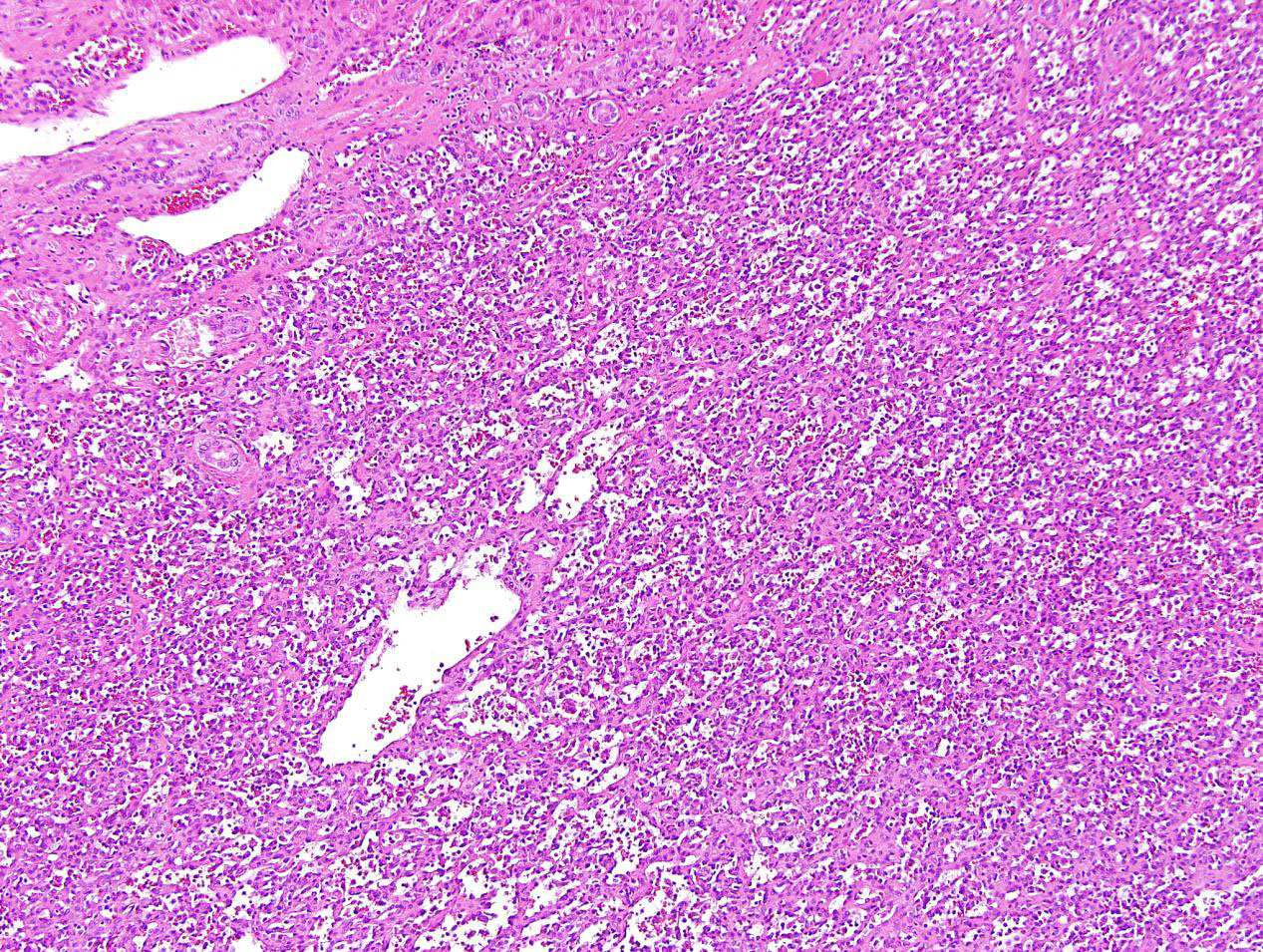 |
| Figure 2 |
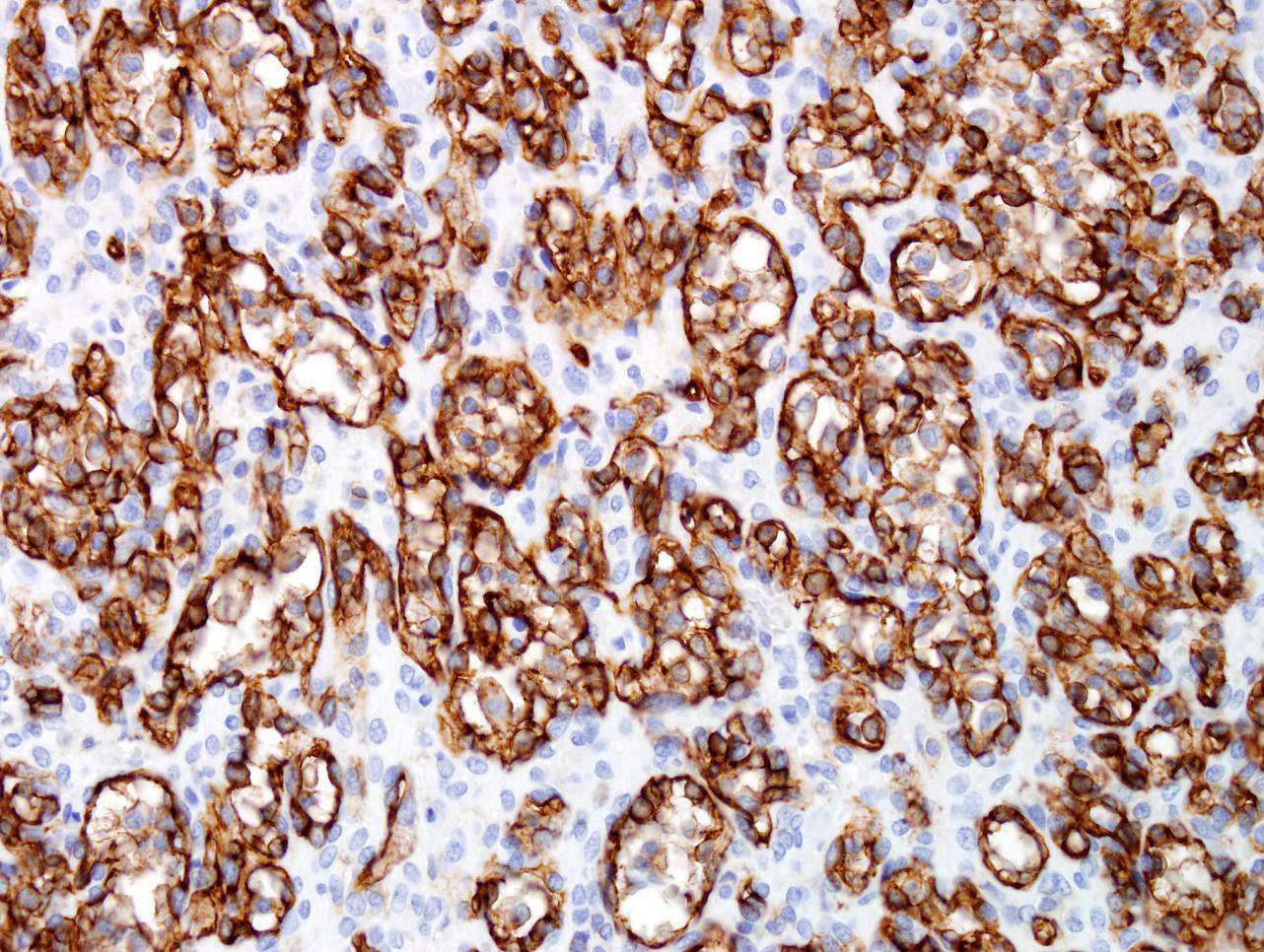 |
| Figure 3, CD31 immunohistochemistry |
Final diagnosis:
Hemangioma, anastomosing type.
Discussion:
Hepatic hemangioma is a common benign vascular neoplasm in both infants and adults that shares the same growth pattern and prognosis as its cutaneous counterpart. Based on its distribution, hemangioma can be classified as focal, multifocal, or diffuse. Most hepatic hemangiomas are of the cavernous type followed by the capillary type. Capillary hemangioma, including lobular capillary hemangioma (also known as pyogenic granuloma) commonly presents on the skin and mucosa, although rare liver or gastrointestinal tract examples have been reported. Capillary hemangioma is composed of a lobular proliferation of vascular channels with plump endothelial cells lining the vascular channels. Anastomosing hemangiomas in the liver, as seen in this case, are rare hepatic vascular neoplasms characterized by an interconnecting sinusoidal-like pattern of tightly packed capillary channels. The tumor appears well circumscribed grossly with a gray-brown focally spongy appearance in the liver. Low-power magnification shows a well-demarcated lesion with lobular architecture in the liver. At higher magnification the tumors consists of anastomosing sinusoidal capillary-sized vessels with scattered hobnail endothelial cells within a framework of non-endothelial supporting cells. No mitotic figures or necrosis are observed. Mild cytologic atypia is appreciated. Immunohistochemical stain for CD31 is diffusely positive.
The primary differential diagnosis of anastomosing hemangioma is angiosarcoma. Angiosarcoma of the liver and gastrointestinal tract is rare and behaves aggressively. The overall survival is poor and patients rapidly develop metastases and usually die within 6–12 months. Accurate diagnosis can be challenging, particularly if the patients have no history of exposure to specific toxins including thorium dioxide, arsenicals, and vinyl chloride monomer. Distinguishing anastomosing hemangioma from a well-differentiated angiosarcoma is challenging especially on small biopsies. Histologically, branching, jagged, slit-like vascular channels with prominent cytological alterations and a diffuse infiltrating border is characteristic of angiosarcoma, in contrast to the sharp demarcation, mild cytological atypia, and lack of mitotic figures in anastomosing hemangioma. The absence of multilayering of endothelial cells, high grade cytologic atypia, and mitotic activity coupled with circumscribed borders favor a benign process. Awareness of this entity and attention to cytological features and the overall lobular architecture are essential to avoid diagnostic errors.
In summary, anastomosing hemangiomas in the liver is a rare entity and leads to concern for angiosarcoma. Awareness of this entity can minimize a misdiagnosis of angiosarcoma and avoid unnecessary aggressive treatment.
References
1. Kulungowski AM, Alomari AI, Chawla A, Christison-Lagay ER, Fishman SJ. Lessons from a liver hemangioma registry: subtype classification. J Pediatr Surg. Jan 2012;47(1):165-170.
2. Dickie B, Dasgupta R, Nair R, et al. Spectrum of hepatic hemangiomas: management and outcome. J Pediatr Surg. Jan 2009;44(1):125-133.
3. Abaalkhail F, Castonguay M, Driman DK, Parfitt J, Marotta P. Lobular capillary hemangioma of the liver. Hepatobiliary Pancreat Dis Int. Jun 2009;8(3):323-325.
4. Nishiyama N, Mori H, Kobara H, et al. Bleeding duodenal hemangioma: morphological changes and endoscopic mucosal resection. World journal of gastroenterology : WJG. Jun 14 2012;18(22):2872-2876.
5. Giaccaglia V, Stefanuto A, Cavallotti C, Quintiliani A, Stipa F. Transanal excision of rectal pyogenic granuloma: case report and literature review. Surg Laparosc Endosc Percutan Tech. Apr 2011;21(2):e91-92.
6. Santos J, Ruiz-Tovar J, Lopez A, Arroyo A, Calpena R. Simultaneous massive low gastrointestinal bleeding and hemoperitoneum caused by a capillary hemangioma in ileocecal valve. International journal of colorectal disease. Oct 2011;26(10):1363-1364.
7. Nagoya H, Tanaka S, Tatsuguchi A, et al. Rare cause of obscure gastrointestinal bleeding due to pyogenic granuloma in the ileum detected by capsule endoscopy and treated with double balloon endoscopy. Dig Endosc. Jan 2010;22(1):71-73.
8. Park SY, Park CH, Lee WS, Kim HS, Choi SK, Rew JS. Pyogenic granuloma of the duodenum treated successfully by endoscopic mucosal resection. Gut Liver. Mar 2009;3(1):48-51.
9. Shibuya T, Osada T, Mitomi H, et al. Jejunal capillary hemangioma treated by using double-balloon endoscopy (with video). Gastrointest Endosc. Sep 2010;72(3):660-661.
10. Benevento A, Boni L, Dionigi G, Besana Ciani I, Danese E, Dionigi R. Multiple hemangiomas of the appendix and liver. J Am Coll Surg. Nov 2003;197(5):860-861.
11. Lin J, Bigge J, Ulbright TM, Montgomery E. Anastomosing hemangioma of the liver and gastrointestinal tract: an unusual variant histologically mimicking angiosarcoma. The American journal of surgical pathology. Nov 2013;37(11):1761-1765.
12. Brown CJ, Falck VG, MacLean A. Angiosarcoma of the colon and rectum: report of a case and review of the literature. Diseases of the colon and rectum. Dec 2004;47(12):2202-2207.
13. Maluf D, Cotterell A, Clark B, Stravitz T, Kauffman HM, Fisher RA. Hepatic angiosarcoma and liver transplantation: case report and literature review. Transplantation proceedings. Jun 2005;37(5):2195-2199.
14. Alrenga DP. Primary angiosarcoma of the liver. Review article. Int Surg. Apr 1975;60(4):198-203.
15. Elliott P, Kleinschmidt I. Angiosarcoma of the liver in Great Britain in proximity to vinyl chloride sites. Occupational and environmental medicine. Jan 1997;54(1):14-18.
16. Bhati CS, Bhatt AN, Starkey G, Hubscher SG, Bramhall SR. Acute liver failure due to primary angiosarcoma: A Case Report and Review of the Literature. World J of Surg Oncol. 2008;6:104.
Contributed by:
Jingmei Lin, MD, PhD
Department of Pathology and Laboratory Medicine
Indiana University School of Medicine