
Interesting Case March 2015
Clinical History
A 30 year old man was referred for liver transplantation workup for presumed liver cirrhosis from NASH. The clinical diagnosis of NASH cirrhosis was based on hepatosplenomegaly, low platelets and steatosis on liver imaging and the local biopsy. The only risk factor for NASH was hypercholesterolemia.
Labs
AST 53 U/L, ALT 87 U/L, ALP 75 U/L, platelets 101,000/µL.
The patient was referred to a liver transplantation center and the biopsy was re-evaluated. Images from the liver biopsy are shown below.
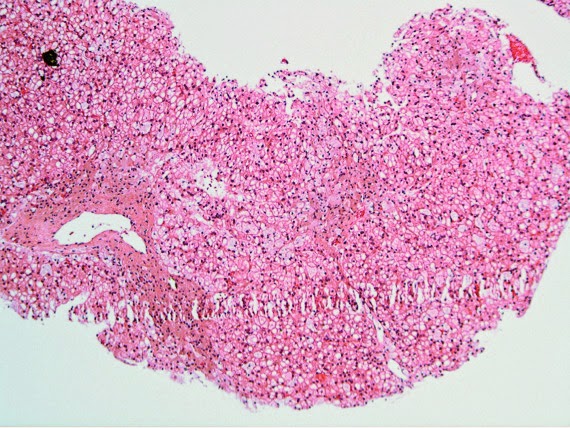
Liver Biopsy Findings
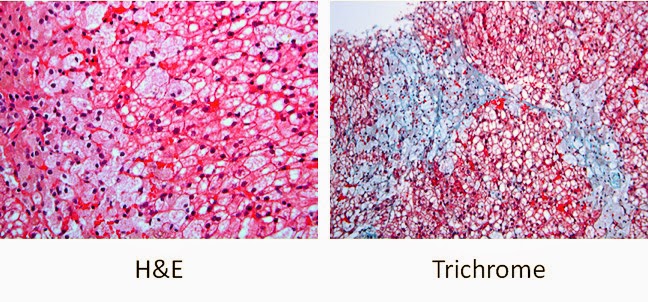
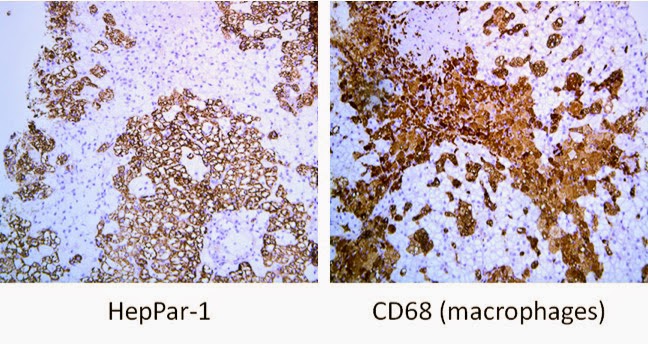
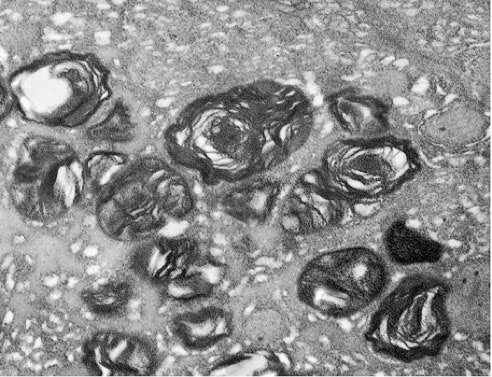
The biopsy shows clusters of “sea-blue” cells that contain pale, foamy cytoplasmic material. These cells stain with the macrophage marker CD68, but not the hepatocyte marker Hep-Par1. The hepatocytes have mild microvesicular steatosis, but no features of steatohepatitis are apparent. Also there is only very little fibrosis. By electron micrograph, the macrophages contain laminated myelin figures.
Diagnosis
Sea blue histocytosis syndrome
Major Learning Points
- Clinical, non-invasive features of cirrhosis and portal hypertension, such as thrombocytopenia, can have other causes.
- Sea-blue histiocytosis (SBH) syndrome can be subtle and not always as prominent as in this case. But SBH syndrome should be kept in mind in certain clinical contexts, including unexplained hepatosplenomegaly.
- The published cases of SBH involving the liver are for the most part due to inherited lysosomal storage disorders. Typically the bone marrow is the most commonly affected organ, baring a few exceptions such as patients receiving fat emulsion in total parenteral nutrition.
- Electron microscopy, though rarely utilized in today’s clinical hepatopathology practice, could play a helpful role in defining the nature of cytoplasmic accumulations.
Discussion
Steatohepatitis is a common disease and it has become a frequent cause of referral to liver transplantation centers. In addition, the proportion of liver transplantations for NASH is projected to increase due the availability of new highly efficacious direct antiviral agents for hepatitis C. It is worth highlighting the need to carefully evaluate the clinical, non-invasive parameters of cirrhosis knowing that these assessments are surrogates and can sometimes produce false positive results. In this patient with an enlarged spleen, low platelets, hyperlipidemia and radiologic diagnosis of “fatty liver”, the clinical assessment had pointed in the direction of NASH-related end-stage liver disease. Ultimately, however, this proved to be a case of Nieman-Pick disease which manifests characteristically as hepatosplenomegaly, low platelets and hypercholesterolemia.
The accumulation of lipid material in macrophages of several organs, including the liver, spleen, bone marrow, and lymph nodes, is sometimes referred to as “sea-blue histocytosis” (SBH). The name initially originated form the appearance of these macrophages when stained with Giemsa/PAS, although in the case described above this stain was not necessary to demonstrate these cells. There are many causes of SBH, but in general, it is a feature of lipid or ceroid storage disorders, and can be primary or secondary. The term was first applied in 1941 in the Swiss literature by Dr. Möschlin and later reported as a syndrome in 1970 by Silverstein et al (N Engl J Med 1970; 282:1-4). The syndrome was attributed to adults with Nieman-Pick disease (NPD) in 1977 by Long et al (Am J Med. 1977;62(4):627-35). NPD was ultimately diagnosed in the patient presented above. Following additional studies, he is believed to have Nieman-Pick disease type B. The SBH syndrome is however not unique to NPD and histopathology lacks the specificity to make an etiologic diagnosis in most cases.
Determining an etiology for SBH syndrome requires the combination of clinical, histopathological, biochemical and genetic information. Some of the other primary/inherited diseases associated with the SBH are cholesterol ester storage disease, Gaucher disease, hypertriglyceridemia (with mutation in the receptor-binding region of the apoE molecule), lecithin-cholesterol acyltransferase deficiency (i.e., Norum disease), ceroid lipofuscinosis and Tangier disease. Several acquired conditions have also been associated SBH, including administration of fat emulsion in total parenteral nutrition, as well as some hematologic conditions. The bone marrow, and less likely the liver, is the usual site of SBH accumulation in these hematologic conditions, such as in myelodysplastic syndrome (J Clin Pathol. 1993 Nov;46(11):1030-2).
Contributed by:
Oyedele Adeyi, MD
Department of Pathology, Toronto General Hospital, Toronto, Ontario.