Clinical history
This biopsy is from a 62 year old male who underwent liver transplantation 6 months prior for decompensated hepatitis C cirrhosis and multifocal hepatocellular carcinoma. Two months prior to this biopsy (4 months post-transplant) the patient’s laboratory studies were abnormal with ALT 57, AST 69, ALP 149, total bilirubin 17.3 mg/dL (296 umol/L) and the liver biopsy at that time showed features consistent with fibrosing cholestatic recurrent hepatitis C. The patient was urgently treated with Simeprevir and Sofosbuvir, in addition to his other medications which included prednisone and Tacrolimus. At the time of this biopsy, two months after commencing HCV treatment, his viral RNA was down to 1 log but his liver enzymes began to rise with mainly a cholestatic pattern with ALT 13 U/L, AST 26 U/L, ALP 1032 U/L, total bilirubin 2.7 mg/dL (46 umol/L). Imaging showed no evidence of bile duct dilatation, however, he was deemed too ill for MRCP or ERCP. A liver biopsy was obtained; representative pictures are shown below.
Microscopic images
 |
| Figure 1 |
 |
| Figure 2 |
 |
| Figure 3A |
 |
| Figure 3B |
 |
| Figure 4 |
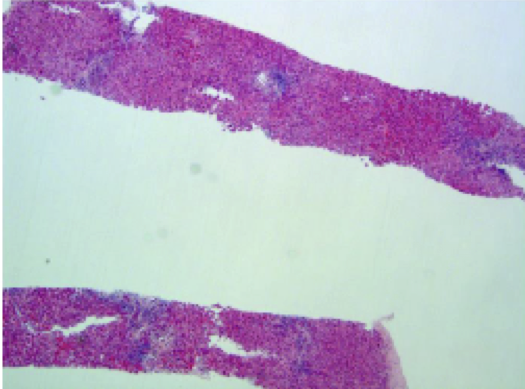
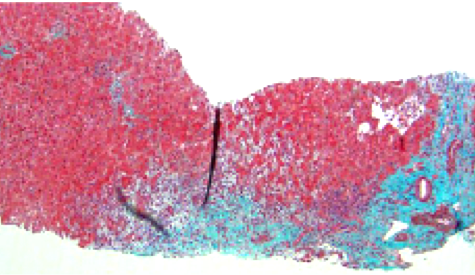
The liver shows mild portal and scanty lobular inflammation (Figure 1-3). The portal tracts, however, are expanded by mild edema, a mild ductular reaction, and the inflammation includes neutrophils. Overall these findings simulate those of biliary obstruction. Fibrosis is mild in the subsinusoidal and periportal areas, but not progressed significantly compared to the biopsy obtained two months earlier. Additionally there is less severe hepatocellular injury compared to the prior biopsy. No viral inclusions are apparent, but occasional foci of neutrophilic microabscesses are identified. The patient was known to have been CMV mismatched with his donor (recipient negative anti-CMV Ab; donor positive). CMV immunohistochemistry was obtained and many cells were positive, most of which were neither “megalic” nor apparent on routine stains, even in hindsight (Figure 4).
Diagnosis
Post-transplant CMV syndrome presenting biochemically and histopathologically as biliary obstruction.
Main Learning Points:
- A combination of immunosuppression, a “sick” patient and unfavorable serology (e.g., CMV recipient-donor mismatch) should always prompt a search for CMV.
- Histopathologically, “classical” CMV inclusions have low sensitivity and are typically rare even in the most severe cases.
- Diagnosis of CMV infection post-transplant therefore depends more on clinical suspicion rather than initial identification of possible viral inclusions.
- In the liver, biliary epithelia are known targets of CMV either directly or indirectly via injury to peribiliary plexus endothelial cells.
- Biliary strictures from mechanical causes are more common than CMV-induced biliary injury, but one should consider CMV infection in the differential diagnosis especially in a suggestive clinical context as described above.
Discussion
With the use of prophylactic and pre-emptive antiviral therapy, cytomegalovirus symptomatic infection now occurs in only about 2-10% of transplanted patients. It usually occurs in the first few months after transplantation and the most important risk factor for the development of the disease is the combination of a seropositive donor with a seronegative recipient. In solid organs transplantation, the graft is particularly prone to infection.
The characteristic and most common histological finding in CMV hepatitis, in our experience, is the presence of neutrophilic aggregates/microabscesses or satellitosis within the parenchyma. Viral inclusions can be seen in hepatocytes, endothelial cells and biliary epithelial cells, but they are often sparse. When suspected, the use of deeper levels and immunohistochemistry should be performed.
CMV infection has been associated with an increased risk for other allograft complications such as chronic rejection and biliary compromise. Biliary complications due to CMV have been reported to occur at a mean post-transplant period of 8.4 months (Liver Transplantation. 2013;19(10):1142-1150), and in this series CMV was detected in the tissues of some patients with undetectable virus in the peripheral blood by PCR. Biliary strictures could also result in part from damage to endothelium of small size hepatic arteries and/or peribiliary plexus.
The histological alterations associated with hepatic CMV infection may cause differential diagnostic problems as inclusions are rarely found. Other infections (bacterial, fungal and viral) or non-infectious conditions (graft ischemia and biliary obstruction) can be associated with neutrophilic microabscesses. Nevertheless a high index of clinical suspicion and occasional neutrophilic microabscesses (arrows in figure 3) in the appropriate clinical setting should prompt immunohistochemistry for the virus. In our practice we tend to order CMV immunohistochemistry on most liver biopsies performed for cause in the first 6 months post-transplant (including liver, bone marrow or other solid organ transplant) irrespective of the clinical presentation. It is also worth noting that inflammation is typically sparse in CMV “hepatitis”. Indeed, abundant inflammation may be indicative of CMV occurring together with some other condition.
In this patient, response to HCV treatment was characterized by improved bilirubin, drop in viral RNA load, and less prominent hepatocellular swelling/disarray. However, CMV PCR in the peripheral blood soon after the second biopsy showed a titer of 4 logs and the CMV titer had been undetectable prior to HCV treatment 2 months earlier. The preceding biopsy had been negative when stained for CMV. The question therefore is: do these new antiviral agents come with increased risk for CMV infection specifically and/or for opportunistic infections in general? The answer is not known but as we gain increasing experience with these drugs, new issues will certainly emerge for the pathologist to consider, and CMV reactivation may be one to keep an eye on. Also the question of a biliary stricture not related to CMV (e.g., anastomotic) cannot be ruled out on the basis of histopathology alone, even with a positive CMV, and the possibility further exploring other causes biliary stricture should be raised.
Case contributed by
Aude Roussel-Jobin, M.D. Fellow, Liver Pathology University of Toronto
References:
Hübscher SG, and Clouston AD, Transplantation pathology. In: Burt A, Portmann L, and Ferrell L, MacSween’s Pathology of the Liver. 6th edition. Churchill Livingstone Elsevier, 2012: 877-878.
Adeyi O, Fischer S and Guindi M. Liver allograft pathology: approach to interpretation of needle biopsies with clinicopathological correlation. J Clin Pathol 2010; 63:47-74.
Gotthardt DN1, Senft J, Sauer P, Weiss KH, et al. Occult cytomegalovirus cholangitis as a potential cause of cholestatic complications after orthotopic liver transplantation? A study of cytomegalovirus DNA in bile. Liver Transpl. 2013;19(10):1142-1150.
Adeyi O. Liver Transplant Pathology. In: Ferrell LD, Kakar S, editors. Consultant Pathology: Liver Pathology. 1st ed. New York City: Demos Medical, 2011:307-342.





