
Interesting Case December 2014 #1
Clinical History:
A 29 year old woman with a 5 year history of insulin dependent diabetes mellitus presented with right flank pain and constipation for the past 2 weeks. During the clinical work up, she was diagnosed with diabetic ketoacidosis and acalculous cholecystitis. Due to elevated liver enzymes and hepatomegaly, liver biopsy was performed during the laparoscopic cholecystectomy.
Labs:
At the time of presentation, the patient’s laboratory values were: blood glucose, 434 mg/dL (normal range [NR] 70-100 mg/dL); alkaline phosphatase, 131 U/L (NR 14-127 U/L); AST, 457 U/L (NR 5-46 U/L); ALT, 230 U/L (NR 4-51 U/L) and total bilirubin, 1.1 mg/dL (NR 0.1-1.5 U/L).
Microscopic Images:
 |
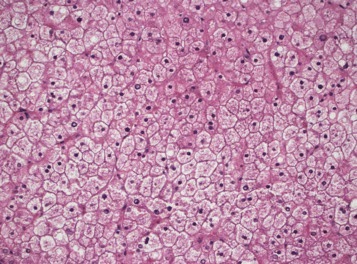
| Figure 1. Low power view showing pale liver parenchyma without steatosis or inflammation. |
 |
| Figure 2. Swollen and rarified hepatocytes with compressed sinusoids. |
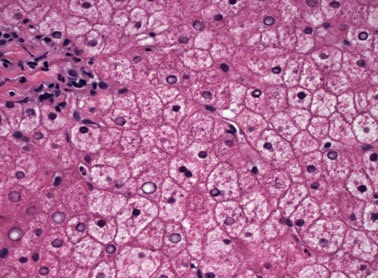 |
| Figure 3. Hepatocytes with multiple giant mitochondria and glycogenated nuclei. |
Diagnosis
Glycogenic Hepatopathy
Discussion
Glycogenic hepatopathy (GH) is not currently commonly seen in practice due to improved diabetic therapies. The typical clinical presentation is elevated blood glucose, elevated liver enzymes, hepatomegaly and abdominal pain. Other signs and symptoms can include abdominal distension, anorexia, nausea, right upper quadrant pain and shortness of breath. The liver biopsy in GH characteristically shows marked accumulation of glycogen in hepatocytes, but the diagnosis requires close clinicopathological correlation.
The pathophysiology of GH is incompletely understood, but it is thought to be caused by prolonged periods of hyperglycemia in poorly controlled diabetic patients treated with insulin. The elevated blood glucose passes into hepatocytes independent of insulin. This is then followed by periods of insulin therapy in which the hepatic glucose is converted to glycogen and the glycogen becomes trapped in hepatocytes. It is thought that the excess hepatic glycogen accumulation leads to hepatocyte injury and causes “leakage” of aminotransferases. Significant hepatocellular death is not typical.
GH also been reported in patients with type II diabetes mellitus, urea cycle defects, and medication effects (e.g., short-term high dose steroids). The differential diagnosis includes hereditary glycogen storage diseases, smooth endoplasmic reticulum proliferation due to medication effects, and glycogen pseudoground glass changes associated with the intake of multiple medications (poly- pharmacotherapy). Rarely GH can coexist with NAFLD or steatohepatitis. Minimal fibrosis has rarely been described in GH; significant fibrosis is not characteristic.
Case contributed by
Jie Ouyang, M.D.
Florida Hospital Center for Diagnostic Pathology
Orlando, Florida