
Interesting Case December 2009
Case History:
58 year old man, previously healthy presented with acute liver failure and is being considered for urgent transplant. Viral serologies (HCV, HBV and HIV) are negative. Imaging studies show a massive liver with question of possible infiltrating neoplasm. Transjugular biopsy obtained as part of transplant workup.
Microscopic Images:
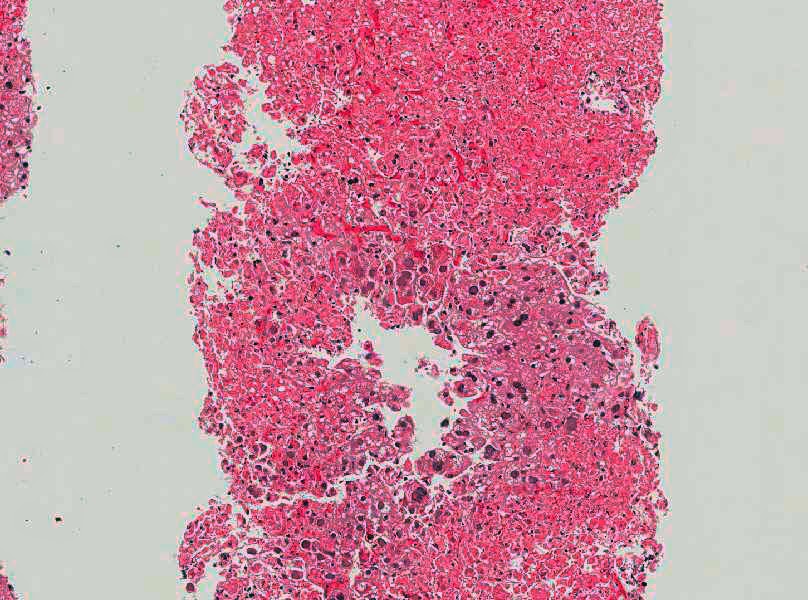 |
| H&E stain |
 |
| H&E stain |
 |
| H&E stain |
Diagnosis:
Herpes simplex viral hepatitis
Discussion:
This is a case or herpes simplex (HSV) hepatitis, confirmed by immunohistochemistry. His prior history revealed nothing to explain a predisposition to this infection. The features in this biopsy are extensive parenchymal necrosis, little inflammation, and characteristic Cowdry type A inclusions in the surviving hepatocytes.
HSV hepatitis is unusual in an immunocompetent host as this patient apparently was, but has been reported (Farr RW, et al. Clin Infect Dis. 1997;24(6):1191-4). Diagnosis is often delayed because of its rarity and because mucocutaneous lesions are often absent. HSV hepatitis can present as multiple hypoechoic nodules in the liver raising neoplasm as a differential (Ak O, et al. Turk J Gastroenterol. 2007;18(2):115-8.) Although treatable, mortality is high and have ranged from 41-79% in some series (Sharma s, et al. J Clin Gastroenterol. 2004;38(8):697-704). Although rare, HSV should be considered in acute hepatitis patients especially when no apparent causes are detected, even if no immunosuppressive state is apparent. Also “nodular lesions” in this context should include HSV hepatitis in the list of differential diagnosis. When such a patient is biopsied showing unexplained parenchymal necrosis, the pathologist should consciously search for viral inclusions which could be rare and require evaluation of multiple levels and immunohistochemistry